kottke.org posts about science
In an incredible effort, science has provided the world with what looks like an incredibly effective vaccine for Covid-19. For Stat, Helen Braswell writes about the challenges of turning that vaccine into vaccinations. In the US, despite heroic work from individuals and individual groups, our public health system has proved unequal to the challenge of addressing the pandemic, and we’re now turning, in part, to that system to distribute and administer the vaccines, as well as to educate the public and drum up support for vaccination. The people that we’re counting on are public officials and healthcare workers worn out from what is essentially one 9-month-long wave of illness, hospitalizations, and death across the country. Misinformation and skepticism of science and government has sowed “justified distrust” about vaccines in many people:
Concern about the vaccines, however, cuts across ethnic and socioeconomic groups. President Trump’s overt efforts to pressure the FDA to issue EUAs before the Nov. 3 election — before the vaccine trials were finished — has deepened the sense of unease. The CDC’s early pandemic testing fiasco, coupled with its sidelining by the Trump administration, has eroded its standing as a trusted source of information.
Alison Buttenheim, an associate professor of nursing and health policy at the University of Pennsylvania, refers to the current situation as a perfect storm of “justified distrust.”
“People who don’t think twice about vaccinating their kids totally on time, who get their flu shot every year, are in the sort of, ‘Hmmm. Might wait six months on this one,’” Buttenheim, who works on vaccine acceptance, told STAT. “I’ve heard people say, ‘I’ll get the European one,’” she said, adding other people have said they would get vaccinated after Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases, gets vaccinated.
And it’s not just the general public. A recent survey of 2,000 doctors and nurses in New Jersey found that 60% of doctors planned to take a Covid vaccine, but only 40% of nurses intended to, Health Commissioner Judith Persichilli said in a recent “60 Minutes” segment about Operation Warp Speed.
Fauci, along with other respected public health officials and workers, should get vaccinated live on CNN. Stream it on YouTube and Twitch. It won’t convert the anti-vax, anti-mask, QAnon wingnuts (nothing will) but if you can at least get healthcare workers and at-risk folks on board, it would be time well spent.
But that’s only one small piece of the puzzle. Braswell’s piece is long and comprehensive look at the challenges regarding the Covid-19 vaccines and is worth reading all the way through.
After Terri Nelson noticed people complaining online about a lack of scent from newly purchased scented candles, Kate Petrova analyzed Amazon reviews for candles from the past three years and found a drop in ratings for scented candles beginning in January 2020 (compared to a smaller ratings decline for unscented candles).
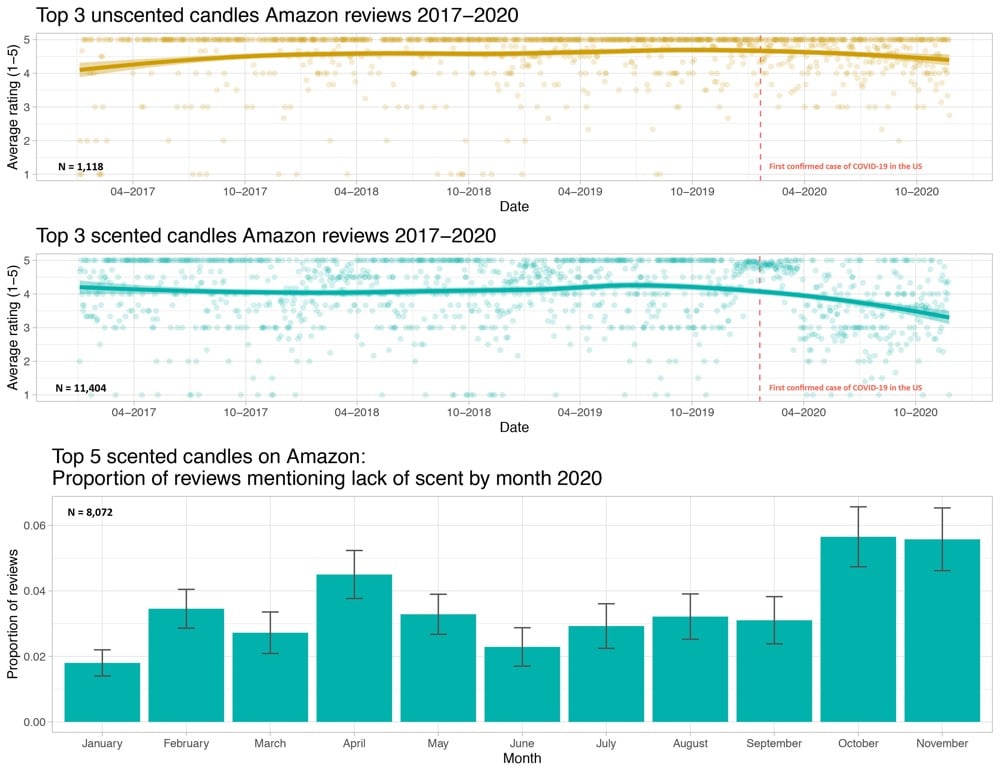
The hypothesis is that some of these buyers have lost their sense of smell due to Covid-19 infections and that’s showing up in the ratings.
With the positive news about the Covid-19 vaccine trials, I assume many of you have started to think about the potential end of the pandemic — what we’ll do, where we’ll go, who we’ll see, and reckon with what’s changed and what’s been lost. I know I have. Alex Hutchinson has written an intriguing piece on what sports science might be able to tell us about the psychology of a situation like the pandemic, where the finish line is poorly defined, ever-changing, or even non-existent.
As it happens, there’s a whole subfield of sports science, at the intersection of physiology and psychology, that explores this terrain. It’s called teleoanticipation, a term coined in 1996 by German physiologist Hans-Volkhart Ulmer to describe how our knowledge of an eventual endpoint (or telos) influences the entirety of an experience. Using endurance sports as their medium, researchers in this subfield have probed what happens when you hide the finish line, surreptitiously move it or take it away entirely. For those of us tempted by promising vaccine updates to start fantasizing about an end to the pandemic, these researchers have some advice: don’t.
Instead, the key seems to be remaining in the moment instead of focusing on the goal.
It turns out that, if you ask yourself “Can I keep going?” rather than “Can I make it to the finish?” you’re far more likely to answer in the affirmative.
This squares with mindfulness practices from Buddhism and Stoicism but also reminds me of a motivational trick I first heard a few years ago: that you can do anything for 10 seconds — and then you just begin a new 10 seconds. Turns out that was popularized by Unbreakable Kimmy Schmidt. Good advice can come from anywhere.
Now that the preliminary results of various Covid-19 vaccine trials are coming out (and looking promising), attention is turning to the eventual distribution of the vaccines. The logistics of getting the doses out to hospitals, clinics, and doctor’s offices is one concern but so is the question of who should get vaccinated first. Supplies of the vaccines will be limited at first, so we’ll need to decide as a society what distribution method is most fair and is of the most benefit to the greatest number of people.
To this end, and in response to a request by the CDC and NIH, the National Academies of Sciences, Engineering, and Medicine formed a committee to produce a report called Framework for Equitable Allocation of COVID-19 Vaccine. The 252-page report is available to the public for free to read online or download.
In addition several recommendations — including that the vaccine be distributed to everyone free of charge — a central feature of the report is a four-phase system of vaccine distribution, summarized in this graphic:
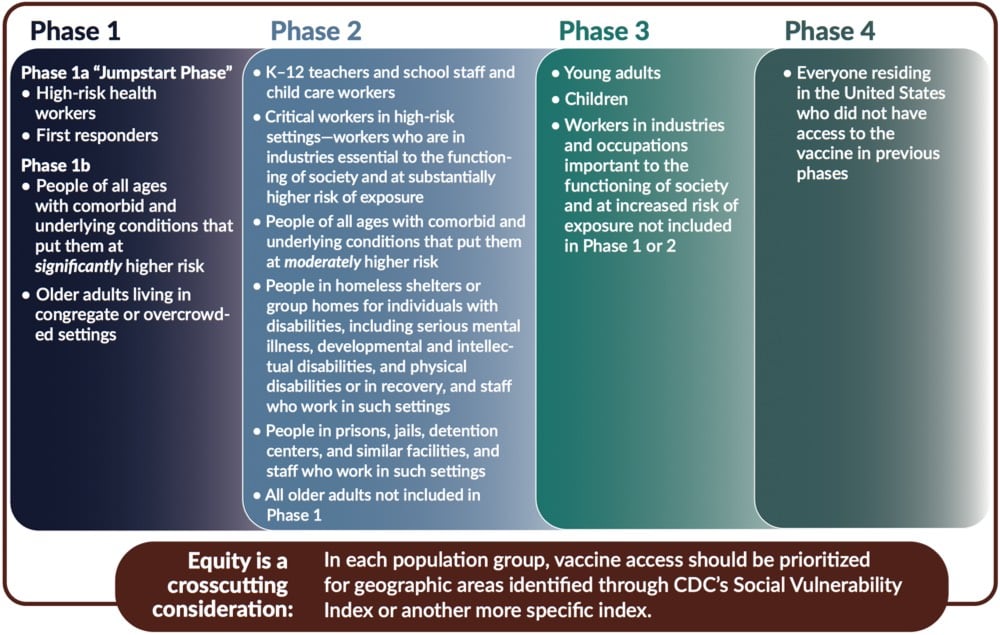
I’d like to stress that this graphic does not show all groups of people included in each phase — please consult the text of the report for that before you go sharing that graphic on social media without context. For example, here’s the full description for “high-risk health workers” in Phase 1a:
This group includes frontline health care workers (who are in hospitals, nursing homes, or providing home care) who either (1) work in situations where the risk of SARS-CoV-2 transmission is higher, or (2) are at an elevated risk of transmitting the infection to patients at higher risk of mortality and severe morbidity. These individuals — who are themselves unable to avoid exposure to the virus — play a critical role in ensuring that the health system can care for COVID-19 patients.
These groups include not only clinicians (e.g., nurses, physicians, respiratory technicians, dentists and hygienists) but also other workers in health care settings who meet the Phase 1a risk criteria (e.g., nursing assistants, environmental services staff, assisted living facility staff, long-term care facility staff, group home staff, and home caregivers). The health care settings employing these workers who are at increased risk of exposure to the virus may also include ambulatory and urgent care clinics; dialysis centers; blood, organ, and tissue donation facilities; and other non-hospital health care facilities. Finally, there are community and family settings where care for infected patients occurs. Not all the workers in these settings are paid for their labor, but, while they are caring for infected people, they all need to be protected from the virus.
Situations associated with higher risk of transmission include caring for COVID-19 patients, cleaning areas where COVID-19 patients are admitted, treated, and housed, and performing procedures with higher risk of aerosolization such as endotracheal intubation, bronchoscopy, suctioning, turning the patient to the prone position, disconnecting the patient from the ventilator, invasive dental procedures and exams, invasive specimen collection, and cardiopulmonary resuscitation. In addition, there are other frontline health care workers who, if they have uncontrolled exposure to the patients or the public in the course of their work, should be in this initial phase. This group includes those individuals distributing or administering the vaccine — especially in areas of higher community transmission — such as pharmacists, plasma and blood donation workers, public health nurses, and other public health and emergency preparedness workers. The committee also includes morticians, funeral home workers, and other death care professionals involved in handling bodies as part of this high-risk group.
The report declines to list specific industries which would be covered in Phase 2’s “critical workers in high-risk settings” but generally says:
The industries in which these critical workers are employed are essential to keeping society and the economy functioning. Since the beginning of the pandemic, millions of people have been going to work and risking exposure to the virus to ensure that markets have food; drug stores have pharmaceutical products; public safety and order are maintained; mail and packages are delivered; and buses, trains, and planes are operating.
Note also the text at the bottom of the graphic: they recommend that within each phase, priority be given to geographic areas where folks are more socially vulnerable in situations like these (e.g. as represented in the CDC’s Social Vulnerability Index).
In developing this phased approach, the committee focused on those who are at the most risk of exposure, severe illness or death, and passing along the virus to others as well as critical workers:
Risk of acquiring infection: Individuals have higher priority to the extent that they have a greater probability of being in settings where SARS-CoV-2 is circulating and of being exposed to a sufficient dose of the virus.
Risk of severe morbidity and mortality: Individuals have higher priority to the extent that they have a greater probability of severe disease or death if they acquire infection.
Risk of negative societal impact: Individuals have higher priority to the extent that societal function and other individuals’ lives and livelihood depend on them directly and would be imperiled if they fell ill.
Risk of transmitting infection to others: Individuals have higher priority to the extent that there is a higher probability of their transmitting the infection to others.
You should read (or at least skim) the full report for more information about the plan and the rationale behind it.
On a personal parting note, as someone who is squarely in the 5-15% of Americans covered in Phase 4 — more specifically: as a 40-something straight white man who non-essentially works from home, isn’t low-income, doesn’t socialize widely even under normal circumstances, and should probably be the very last person on this whole Earth scheduled to be vaccinated under an equitable framework — I am content to wait my turn should the US adopt this framework or something like it.1 Distributing vaccines to those who need them most is absolutely the right thing to do, both ethically and from the standpoint of getting society “back to normal” as quickly as possible and with as little additional death and suffering as possible.
Preliminary results from the trials of the Covid-19 vaccine jointly developed by the University of Oxford and AstraZeneca indicate that the vaccine’s overall efficacy is 70% but that a regimen that calls for a lower first dose is 90% effective.
The preliminary results on the AstraZeneca vaccine were based on a total of 131 Covid-19 cases in a study involving 11,363 participants. The findings were perplexing. Two full doses of the vaccine appeared to be only 62% effective at preventing disease, while a half dose, followed by a full dose, was about 90% effective. That latter analysis was conducted on a small subset of the study participants, only 2,741.
Hopefully more study will be done on that dosage question. From the AP:
“The report that an initial half-dose is better than a full dose seems counterintuitive for those of us thinking of vaccines as normal drugs: With drugs, we expect that higher doses have bigger effects, and more side-effects,” he said. “But the immune system does not work like that.”
The seemingly lower efficacy comes with some perhaps significant benefits: this vaccine is cheaper to produce and doesn’t require any special refrigeration.
The vaccine can be transported under “normal refrigerated conditions” of 2 to 8 degrees Celsius (36 to 46 degrees Fahrenheit), AstraZeneca said. By comparison, Pfizer plans to distribute its vaccine using specially designed “thermal shippers” that use dry ice to maintain temperatures of minus-70 degrees Celsius (minus-94 degrees Fahrenheit).
The Pfizer and Moderna vaccines were pretty similar in many respects and this one seems quite different. These results were just released a few hours ago, so it will be interesting to follow the debate and expert commentary on this. Stay tuned…
Update: This is amazing: the seemingly more effective 1/2 dose + full dose regimen was a mistake.
Around the time when Astra was initiating its partnership with Oxford at the end of April, university researchers were administering doses to trial participants in Britain.
They soon noticed expected side effects such as fatigue, headaches or arm aches were milder than expected, he said.
“So we went back and checked … and we found out that they had underpredicted the dose of the vaccine by half,” said Pangalos.
A far smaller number of participants was given the initial half-dose, so more research will need to be done to determine if this mistake will be added to the long list of scientific discoveries made because of errors. There’s a good piece in Nature that talks about what we know and don’t know about the vaccine results so far along with some informed speculation.
But, if the differences are bona fide, researchers are eager to understand why. “I don’t think it’s an anomaly,” says Katie Ewer, an immunologist at Oxford’s Jenner Institute who is working on the vaccine. “I’m keen to get into the lab and start thinking about how we address that question.” She has two leading theories for why a lower first dose might have led to better protection against COVID. It’s possible that lower doses of vaccine do a better job at stimulating the subset of immune cells called T cells that support the production of antibodies, she says.
Another potential explanation is the immune system’s response against the chimpanzee virus. The vaccine triggers an immune response not only to the SARS-CoV-2 spike protein, but also to components of the viral vector. It’s possible that the full first dose blunted this reaction, says Ewer. She plans to look at antibody responses against the chimpanzee virus to help address this question.
Update: A short thread by Dr. Natalie Dean, which leads with “AstraZeneca/Oxford get a poor grade for transparency and rigor when it comes to the vaccine trial results they have reported”.
For Vox, Julia Belluz takes a look at the approach that’s made Vermont more successful than most other US states in combatting Covid-19. The big thing? State officials recognized that those most at risk needed more support.
There’s a fatal flaw embedded in the basic Covid-19 test, trace, and isolate trifecta used around the world: It doesn’t account for the fact that the coronavirus is not an equal-opportunity pathogen. The people who are most likely to be tested, and to have the easiest time quarantining or isolating, are also the least likely to get sick and die from the virus.
From the United Kingdom to Sweden to Canada, we have evidence that the virus preys on people employed in “essential service” jobs (bus drivers, nurses, factory workers), which don’t allow for telecommuting or paid sick leave; people in low-income neighborhoods; and people in “congregate housing” like shelters, prisons, and retirement homes.
People of color tend to be overrepresented in these groups — but there’s no biological reason they’re more likely to get sick and die from the virus. Simply put: They tend to work jobs that bring them outside the home and into close contact with other people, live in crowded environments ideal for coronavirus contagion, or both.
The state then directed efforts, resources, and money to nursing homes, the unhoused, prisons, and essential workers to make it easier for those folks to stay safe.
I also thought this bit was really interesting:
There’s a simple adage in public health: “Never do a test without offering something in exchange,” said Johns Hopkins’s Stefan Baral. So when a patient gets tested for HIV, for example, they’re offered treatment, support, or contact tracing. “We’re not just doing the testing to get information but also providing a clear service,” Baral added, and potentially preventing that person from spreading the virus any further. “This is basic public health.”
With Covid-19, the US has failed at basic public health. Across the country, people have been asked to get tested without anything offered in exchange.
“If we are asking people to stay home and not work, we have to make sure society is supporting them,” Baral said. “An equitable program would support people to do the right thing.”
“Never do a test without offering something in exchange.” To the extent that federal and state governments have been asking to people to stay home, get tested, and wear a mask, many of those same governments have been unwilling or unable to provide people with much in return for doing so. And so, here we are months into this, paying for that inaction with 250,000 lives.
Update: How NYC does “never do a test without offering something in exchange”:
You can access a free hotel room to safely isolate from your family, which include meals, Rx delivery, free wi-fi, medical staff on site, and transportation to and from hotel and medical appointments.
(via @agoX)
As I write this, it’s snowing outside here in Vermont and Covid-19 has finally gained a foothold in our little state. At the governor’s press conference yesterday, he and his pandemic response team announced that contact tracing done by the state showed that the rise in cases started as an outbreak in some hockey leagues. That initial outbreak wasn’t contained and subsequent non-essential, indoor, mask-less, multi-household gatherings and Halloween parties resulted in the very sharp rise we started to see here in the first week of November.
Scott explained that 71% of outbreaks reported from Oct. 1 to Nov. 13 were linked to “social events, parties and people hanging out at home or bars and clubs.” He added Vermont has not seen the virus spread widely at schools, restaurants or other businesses.
Dr. Mark Levine, the state health commissioner, said those parties came in a variety of sizes of parties — Halloween gatherings large and small, dinner parties, baby showers, “people in the high single numbers at a deer camp.”
In states with many infections, particularly in the Midwest, contact tracing is all but impossible, so it’s instructive to pay attention to Vermont’s example here: we’re doing the tracing and the tracers say the infections are coming from people gathering indoors across multiple households. Which is exactly what public health and medical experts have been urging people not to do for months now.
And that brings us to Thanksgiving. For The Atlantic, Rachel Gutman asked her colleagues who have been writing extensively about the pandemic for some of their top safety rules and guidelines and their number one was, say it with me:
My colleagues’ guidance boils down to this winter’s golden rule for interacting with anyone outside your immediate household: Don’t spend time indoors with other people.
Here it is again in a fun font, just to make sure you got it: 𝓓𝓸𝓷’𝓽 𝓼𝓹𝓮𝓷𝓭 𝓽𝓲𝓶𝓮 𝓲𝓷𝓭𝓸𝓸𝓻𝓼 𝔀𝓲𝓽𝓱 𝓸𝓽𝓱𝓮𝓻 𝓹𝓮𝓸𝓹𝓵𝓮.
Look, for some people spending time indoors with others is essential — jobs, education, etc. — but those who don’t have to, shouldn’t. And this goes for everywhere in the US because no states (aside from maybe Hawaii) are doing well right now — cases are either high, rising sharply, or both. Please please don’t gather in indoor, multi-household groups for Thanksgiving if you haven’t quarantined beforehand. In the US right now, about 1-in-55 people who get Covid-19 die from it. With rates already high around the country, if many people do Thanksgiving as usual, an already horrific and deadly situation could become much much worse.
According to an unpublicized report by the Chinese government, the first documented case of Covid-19 was a 55-year-old person living in Hubei province on November 17, 2019. That makes today the first anniversary of the start of the Covid-19 pandemic. From that person (and possibly earlier or concurrent cases), the disease slowly and silently spread until it was determined to be due to a novel coronavirus.
They found that following the Nov. 17 case, about one to five new cases were reported every day and by Dec. 15, the total infections reached 27. Daily cases seem to have increased after that, with the case count reaching 60 by Dec. 20, the SCMP reported.
On Dec. 27, Dr. Zhang Jixian, head of the respiratory department at Hubei Provincial Hospital, reported to health officials in China that a novel coronavirus was causing the disease; by that day, it had infected more than 180 individuals. (Doctors may not have been aware of all of those cases at the time, but only identified those cases after going back over the records, the Morning Post reported.)
No one had any idea how much the world was going to change that day. What an awful, humbling, terrifying, ghoulish year.
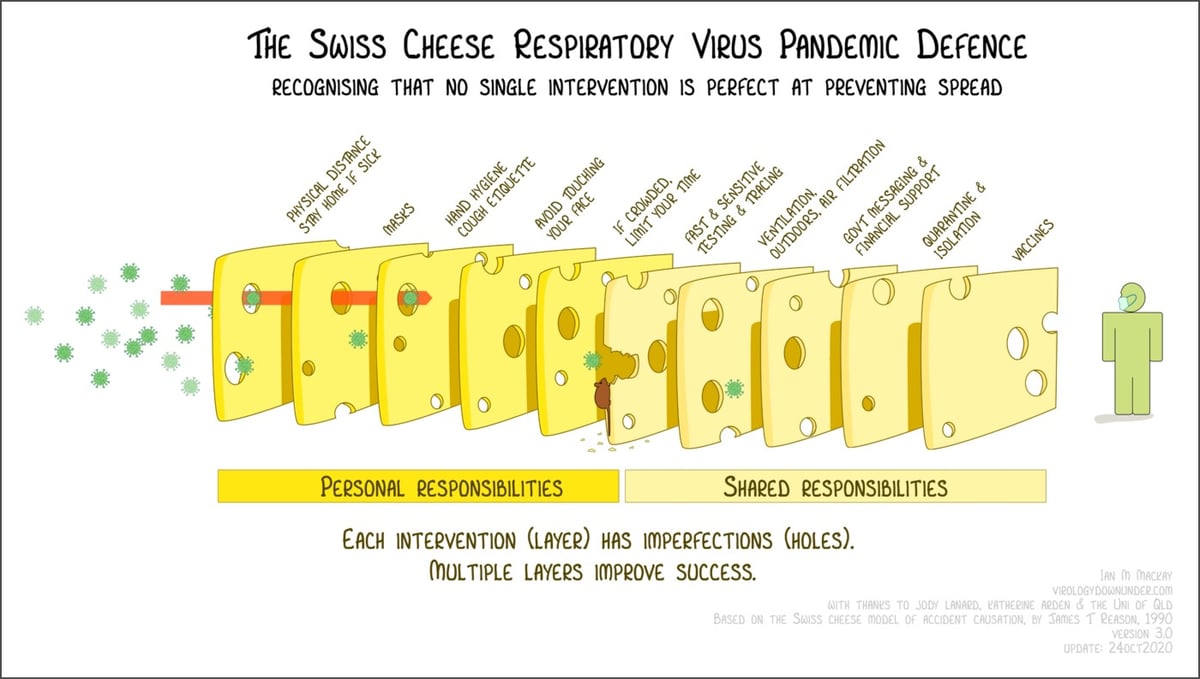
The Swiss cheese model of accident causation is a framework for thinking about how to layer security measures to minimize risk and prevent failure. The idea is that when several layers of interventions, despite their weaknesses, are properly stacked up between a hazard and a potentially bad outcome, they are able to cumulatively prevent that outcome because there’s no single point of failure. During the pandemic, health care workers and public health officials have been using the Swiss cheese model to visualize how various measures can work together to help keep people safe.
Virologist Dr. Ian Mackay has visualized the Swiss cheese Covid-19 defense in a wonderful way (pictured above). Each layer of cheese represents a personal or shared intervention — like mask wearing, limiting your time indoors w/ crowds, proper ventilation, quarantine, vaccines — and the holes are imperfections. Applied together, these imperfect measures work like a filter and can vastly improve chances of success.1 He even added a “misinformation mouse” chewing through one of the cheese slices to represent how deceptive information can weaken these defenses.
Mackay has released this graphic under a Creative Commons license (free to share and adapt w/ attribution) and is available in English, German, French, Spanish, Korean, and several other languages. (via @EricTopol)
Zeynep Tufekci says that a devastating third pandemic surge is upon us and that It’s Time to Hunker Down. She leads with the good news (vaccines, treatments, knowledge, testing capacity & quickness) but notes that with winter coming and a high baseline of cases from a summer not spent in preparation, now is the time to really knuckle down so that we can get to the finish line.
Whatever the causes, public-health experts knew a fall and winter wave was a high likelihood, and urged us to get ready.
But we did not.
The best way to prepare would have been to enter this phase with as few cases as possible. In exponential processes like epidemics, the baseline matters a great deal. Once the numbers are this large, it’s very easy for them to get much larger, very quickly — and they will. When we start with half a million confirmed cases a week, as we had in mid-October, it’s like a runaway train. Only a few weeks later, we are already at about 1 million cases a week, with no sign of slowing down.
Americans are reporting higher numbers of contacts compared with the spring, probably because of quarantine fatigue and confusing guidance. It’s hard to keep up a restricted life. But what we’re facing now isn’t forever.
It’s time to buckle up and lock ourselves down again, and to do so with fresh vigilance. Remember: We are barely nine or 10 months into this pandemic, and we have not experienced a full-blown fall or winter season. Everything that we may have done somewhat cautiously — and gotten away with — in summer may carry a higher risk now, because the conditions are different and the case baseline is much higher.
On Friday, November 13, 170,792 new cases of Covid-19 were reported in the United States. About 3000 of those people will die from their disease on Dec 6 — one day of Covid deaths equal to the number of people who died on 9/11. It’s already baked in, it’s already happened. Here’s how we know.
The case fatality rate (or ratio) for a disease is the number of confirmed deaths divided by the number of confirmed cases. For Covid-19 in the United States, the overall case fatality rate (CFR) is 2.3%. That is, since the beginning of the pandemic, 2.3% of those who have tested positive for Covid-19 in the US have died. In India, it’s 1.5%, Germany is at 1.6%, Iran 5.5%, and in Mexico it’s a terrifying 9.8%.
A recent analysis by infectious disease researcher Trevor Bedford tells us two things related to the CFR.
1. Reported deaths from Covid-19 lag behind reported cases by 22 days. Some deaths are reported sooner and some later, but in general it’s a 22-day lag.1
2. The overall CFR in the US is 2.3% but if you use the 22-day lag to calculate what Bedford calls “a lag-adjusted case fatality rate”, it’s a pretty steady average of 1.8% since August. Here’s a graph:
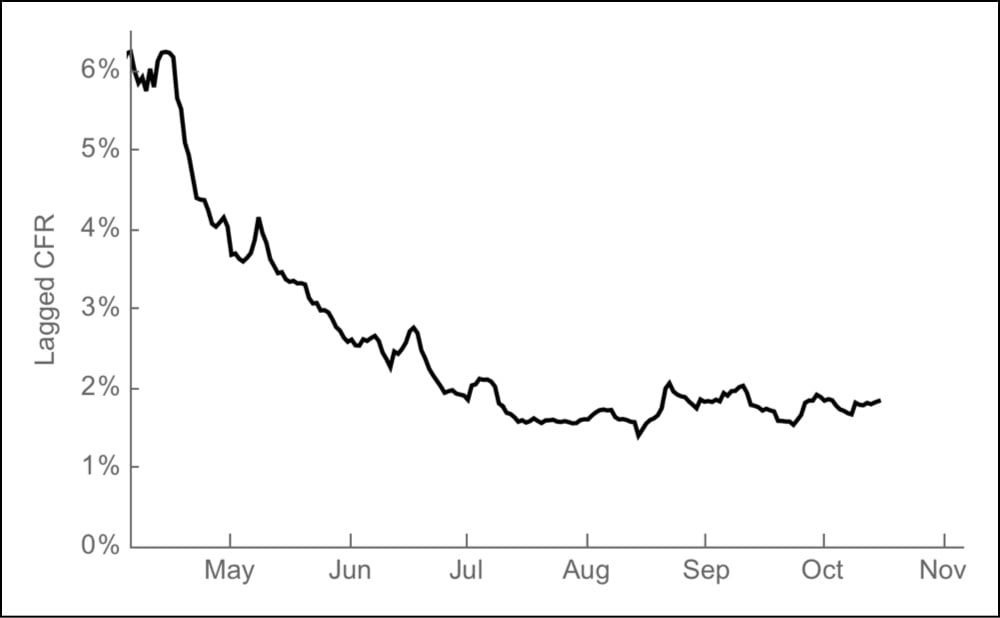
As you can see, in the early days of the pandemic, 4-6% of the cases ended in death and now that’s down to ~1.8%. That’s good news! The less good news is that the current case rate is high and rising quickly. Because of the lag in reported deaths, the rise in cases might not seem that alarming to some, even though those deaths will eventually happen. What Bedford’s analysis provides is a quick way to estimate the number of deaths that will occur in the future based on the number of cases today: just multiply the number of a day’s cases by 1.8% and you get an estimated number of people who will die 22 days later.2
For instance, as I said above, 170,792 cases were reported on Nov 13 — 1.8% is 3074 deaths to be reported on December 6. Cases have been over 100,000 per day for 11 days now: here are the estimated deaths from that time period:
| Date |
Cases |
Est. deaths (on date) |
| 2020-11-15 | 145,670 | 2622 (2020-12-08) |
| 2020-11-14 | 163,473 | 2943 (2020-12-07) |
| 2020-11-13 | 170,792 | 3074 (2020-12-06) |
| 2020-11-12 | 150,526 | 2709 (2020-12-05) |
| 2020-11-11 | 144,499 | 2601 (2020-12-04) |
| 2020-11-10 | 130,989 | 2358 (2020-12-03) |
| 2020-11-09 | 118,708 | 2137 (2020-12-02) |
| 2020-11-08 | 110,838 | 1995 (2020-12-01) |
| 2020-11-07 | 129,191 | 2325 (2020-11-30) |
| 2020-11-06 | 125,252 | 2255 (2020-11-29) |
| 2020-11-05 | 116,153 | 2091 (2020-11-28) |
| 2020-11-04 | 103,067 | 1855 (2020-11-27) |
| Totals | 1,609,158 | 28,965 |
Starting the day after Thanksgiving, a day traditionally called Black Friday, the 1.6 million positive cases reported in the past 12 days will result in 2-3000 deaths per day from then into the first week of December. Statistically speaking, these deaths have already occurred — as Bedford says, they are “baked in”. Assuming the lagged CFR stays at ~1.8% (it could increase due to an overtaxed medical system) and if the number of cases keeps rising, the daily death toll would get even worse. As daily case totals are reported, you can just do the math yourself:
number of cases × 0.018
200,000 cases in a day would be ~3600 deaths. 300,000 daily cases, a number that would have been inconceivable to imagine in May but is now within the realm of possibility, would result in 5400 deaths in a single day. Vaccines are coming, there is hope on the horizon. But make no mistake: this is an absolute unmitigated catastrophe for the United States.
Update: Over at The Atlantic, Alexis Madrigal and Whet Moser took a closer look at Bedford’s model, aided by Ryan Tibshirani’s analysis.
Tibshirani’s first finding was that the lag time between states was quite variable-and that the median lag time was 16 days, a lot shorter than the mean. Looking state by state, Tibshirani concluded, it seemed difficult to land on an exact number of days as the “right” lag “with any amount of confidence,” he told us. Because cases are rising quickly, a shorter lag time would mean a larger denominator of cases for recent days — and a lower current case-fatality rate, something like 1.4 percent. This could mean fewer overall people are dying.
But this approach does not change the most important prediction. The country will still cross the threshold of 2,000 deaths a day, and even more quickly than Bedford originally predicted. Cases were significantly higher 16 days ago than 22 days ago, so a shorter lag time means that those higher case numbers show up in the deaths data sooner. Even with a lower case-fatality rate, deaths climb quickly. Estimating this way, the country would hit an average of 2,000 deaths a day on November 30.
The other major finding in Tibshirani’s analysis is that the individual assumptions and parameters in a Bedford-style model don’t matter too much. You can swap in different CFRs and lag-time parameters, and the outputs are more consistent than you might expect. They are all bad news. And, looking retrospectively, Tibshirani found that a reasonable, Bedford-style lagged-CFR model would have generated more accurate national-death-count predictions than the CDC’s ensemble model since July.
Last Monday the world got some good news: an early review of the data showed that Pfizer’s Covid-19 vaccine was “more than 90% effective” in preventing the disease. The results pointed to other vaccines also being highly effective against the virus and this morning comes this news: Early Data Show Moderna’s Coronavirus Vaccine Is 94.5% Effective.
The drugmaker Moderna announced on Monday that its coronavirus vaccine was 94.5 percent effective, based on an early look at the results from its large, continuing study.
Researchers said the results were better than they had dared to imagine. But the vaccine will not be widely available for months, probably not until spring.
Despite the delivery timeline, this is such good news.
The companies’ products open the door to an entirely new way of creating vaccines — and creating them fast. Both use a synthetic version of coronavirus genetic material, called messenger RNA or mRNA, to program a person’s cells to churn out many copies of a fragment of the virus. That fragment sets off alarms in the immune system and stimulates it to attack, should the real virus try to invade. Although a number of vaccines using this technology are in development for other infections and cancers, none have yet been approved or marketed.
“The fact that two different vaccines made by two different companies with two different kinds of structures, in a new messenger RNA concept, both worked so effectively confirms the concept once and for all that this is a viable strategy not only for Covid but for future infectious disease threats,” said Dr. Barry R. Bloom, a professor of public health at Harvard.
Natalie E. Dean, a biostatistician at the University of Florida, said an important finding was that the vaccine appeared to prevent severe disease. Pfizer did not release information about disease severity when reporting its results.
Researchers say the positive results from Pfizer and Moderna bode well for other vaccines, because all of the candidates being tested aim at the same target - the so-called spike protein on the coronavirus that it uses to invade human cells.
It’s only a few more months — please please do what you can to stay safe and keep others safe (especially medical workers) until these vaccines can be rolled out.
This morning, the transition team for President-elect Joe Biden announced the members of his Covid-19 task force.
The list includes Rick Bright, the former head of the vaccine-development agency BARDA ousted by the Trump administration in April; Atul Gawande, the surgeon, writer, and recently departed CEO of Haven, the joint JP Morgan Chase-Berkshire Hathaway-Amazon health care venture; and Luciana Borio, a former Food and Drug Administration official and biodefense specialist.
Biden has cast the escalating Covid-19 crisis as a priority for his incoming administration. The task force, he said, would quickly consult with state and local health officials on how to best prevent coronavirus spread, reopen schools and businesses, and address the racial disparities that have left communities of color harder hit than others by the pandemic.
From Biden’s transition website, here’s the Biden-Harris administration’s seven-point plan to beat COVID-19 (which is the first item in the site’s “Priorities” menu). The seven points are:
- Ensure all Americans have access to regular, reliable, and free testing.
- Fix personal protective equipment (PPE) problems for good.
- Provide clear, consistent, evidence-based guidance for how communities should navigate the pandemic — and the resources for schools, small businesses, and families to make it through.
- Plan for the effective, equitable distribution of treatments and vaccines - because development isn’t enough if they aren’t effectively distributed.
- Protect older Americans and others at high risk.
- Rebuild and expand defenses to predict, prevent, and mitigate pandemic threats, including those coming from China.
- Implement mask mandates nationwide by working with governors and mayors and by asking the American people to do what they do best: step up in a time of crisis.
This looks like what the plan should have been from the beginning. Of particular note, under the point about testing:
Stand up a Pandemic Testing Board like Roosevelt’s War Production Board. It’s how we produced tanks, planes, uniforms, and supplies in record time, and it’s how we will produce and distribute tens of millions of tests.
Establish a U.S. Public Health Jobs Corps to mobilize at least 100,000 Americans across the country with support from trusted local organizations in communities most at risk to perform culturally competent approaches to contact tracing and protecting at-risk populations.
Over the past week, as Americans voted and then held their breath for the results of the election, over 750,000 Americans tested positive for Covid-19. Based on the current case fatality rate of 2.4%, over 18,000 of those people will die in the days and weeks ahead. Many more will suffer long-term health effects because of the disease and struggle emotionally, financially, and spiritually in the months ahead. I really really hope there’s enough of a spirit of togetherness and cooperation left in America for a science-based plan like this to work in controlling a disease that’s killed almost 230,000 people. We — all Americans — need this so so much.
In a press release (and not a paper in a peer-reviewed journal) based on a preliminary outside review of data from its phase 3 trial, Pfizer says its Covid-19 vaccine was more than 90% effective in preventing the disease.
The company said that the analysis found that the vaccine was more than 90 percent effective in preventing the disease among trial volunteers who had no evidence of prior coronavirus infection. If the results hold up, that level of protection would put it on par with highly effective childhood vaccines for diseases such as measles. No serious safety concerns have been observed, the company said.
I really hope this analysis holds up when more data from the study is released:
The data released by Pfizer Monday was delivered in a news release, not a peer-reviewed medical journal. It is not conclusive evidence that the vaccine is safe and effective, and the initial finding of more than 90 percent efficacy could change as the trial goes on.
The world, and the United States, could really really use some good news like this about the pandemic.
Update: Here’s Pfizer’s press release. And a thread from Dr. Natalie Dean on how she is interpreting this news (“Celebrate, but let the process play out over time as intended.”)
Pfizer’s first analysis was planned for 32 events, which they pushed back after discussions with FDA. But by the time they analyzed the data, 94 had accrued. This shows how quickly trials can generate results when placed in hotspots (and how much transmission is ongoing!).
These vaccines are tested until a certain number of infections happen. So you have this interesting paradoxical situation where if a potential vaccine is more successful at curbing infection, the longer it takes for the study to conclude. You get a better vaccine but wait longer for it. Countering that are the rising transmission counts in the US — more community transmission will get you to the target number of infections more quickly.
Update: From virologist Dr. Florian Krammer, a thread about what Pfizer and other companies will be looking for in terms of the efficacy of vaccines in a number of different situations. Overall, he is optimistic about these preliminary results. And here’s a FAQ about the vaccine from the NY Times.
Another open question is whether children will get protection from the vaccine. The trial run by Pfizer and BioNTech initially was open to people 18 or older, but in September they began including teenagers as young as 16. Last month, they launched a new trial on children as young as 12 and plan to work their way to younger ages.
Update: A very simplified explanation of Pfizer’s RNA-based vaccine.
Let’s say the Earth turned into a black hole. What would happen to someone standing on the surface and for how long would it happen? From Ethan Siegel:
As spectacular as falling into a black hole would actually be, if Earth spontaneously became one, you’d never get to experience it for yourself. You’d get to live for about another 21 minutes in an incredibly odd state: free-falling, while the air around you free-fell at exactly the same rate. As time went on, you’d feel the atmosphere thicken and the air pressure increase as everything around the world accelerated towards the center, while objects that weren’t attached to the ground would appear approach you from all directions.
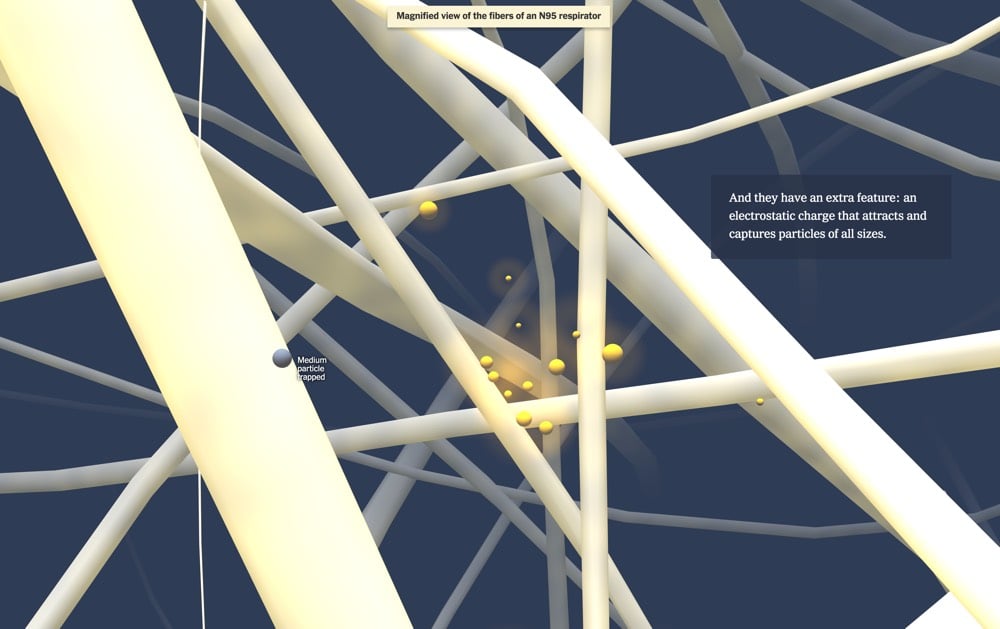
The NY Times has a fantastic visualization on how face masks help keep us safe from catching Covid-19 by taking readers on a journey through a mask to see how they block aerosols and droplets.
A lot of the pushback around the efficacy of masks from non-scientists focuses on the size of the droplets and aerosols (super tiny) compared to the gaps between the fibers in the masks (relatively large). Intuitively, it seems like masks don’t stand a chance of stopping anything. But as this visualization shows, multiple layers of fibers do the job quite well. Masks don’t work like sieves, which will let every particle smaller than the holes through the mesh. Instead, imagine shooting a BB gun into a thick stand of trees — no one tree stands a good chance of getting hit by the BB but the forest will stop it eventually.
N95, KN95, and masks made from polypropylene have an extra weapon against particles: the fibers carry an electrostatic charge that attracts particles to trap them. Picture our BB flying through a forest of magnetic trees — it’s got a much better chance of being captured that way.
The visualization also touches on the importance of making sure your mask fits properly. The best masks fit tightly around the edges and include a space around your nose and nostrils. Masks with unfiltered valves should not be used — you’re just breathing virus out into the air. It’s been 8-9 months now that we’ve been dealing with the pandemic and there will be many more months of wearing masks. If your mask is fits poorly around your nose, your straps aren’t tight enough, you need to fuss with it after putting it on, have a mask with a valve, or (god forbid) are still just wearing a bandana, please please do yourself and others a favor and upgrade your mask. High-quality, well-made masks are much easier to find now than 6-8 months ago.1 If you can’t afford a proper mask, email me and I’ll buy you one. Masks are one of the most successful low-tech interventions we can do to prevent the spread of Covid-19, and the better our masks, the more effective they will be.
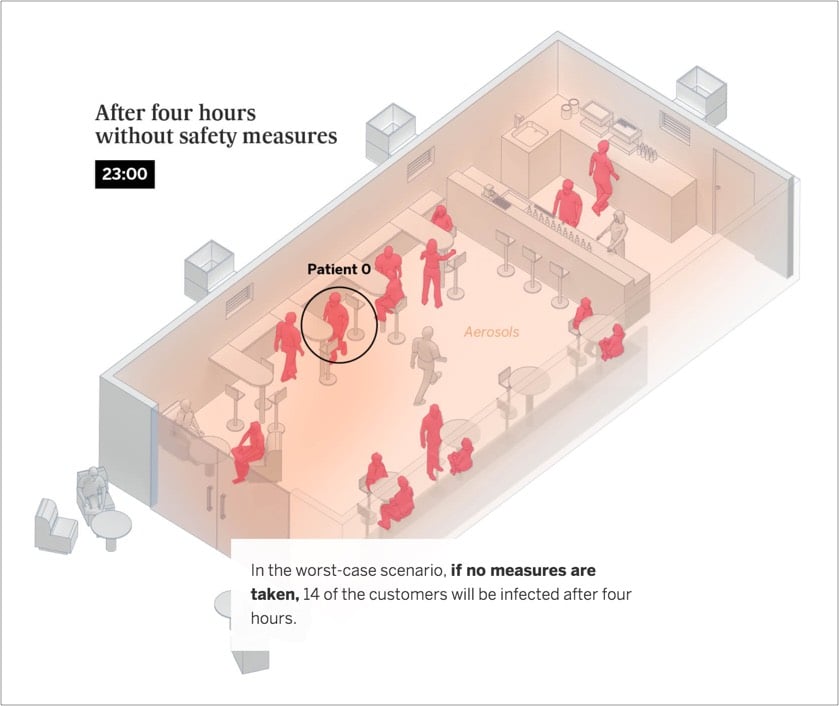
From El Pais, this is an excellent visualization of how Covid-19 spreads indoors via aerosols and what can be done to limit that spread. They go through simulations of three different indoor scenarios that are based on actual events — in a home with friends, in a bar at 50% capacity, and in a classroom — and see what happens when differing levels of precautions are applied: masks, ventilation, and limiting exposure time.
Six people get together in a private home, one of whom is infected. Some 31% of coronavirus outbreaks recorded in Spain are caused by this kind of gathering, mainly between family and friends.
Irrespective of whether safe distances are maintained, if the six people spend four hours together talking loudly, without wearing a face mask in a room with no ventilation, five will become infected, according to the scientific model explained in the methodology.
If face masks are worn, four people are at risk of infection. Masks alone will not prevent infection if the exposure is prolonged.
The risk of infection drops to below one when the group uses face masks, shortens the length of the gathering by half and ventilates the space used.
In all three scenarios, note that distancing is largely irrelevant when people gather indoors for longer periods in poorly ventilated areas. From the school example:
In real outbreaks, it has been noted that any of the students could become infected irrespective of their proximity to the teacher as the aerosols are distributed randomly around the unventilated room.
The only thing that’s disappointing about this piece is that it does not stress enough that finding alternatives to indoor activities with lots of people is the much safer course of action than just cracking a window or masking up. Safety step #1 is still being smart about non-essential activities — masks and ventilation are not magically going to protect you during risky activities. Educating our children is important and difficult (though not impossible) to do outside in many places, so yeah, let’s mask up and ventilate those classrooms. But your indoor birthday party with 10 friends or Thanksgiving dinner with the cousins and grandparents? Or dining out in a room full of strangers at a restaurant? Even with masks and ventilation, it’s not a great idea. Scale it down, move it to Zoom/FT, hold it outdoors (distanced, masked), or just skip it.

Using the Dark Energy Camera at the Cerro Tololo observatory in Chile, astronomers took an image of the stars clustered around the center of our Milky Way galaxy that shows about 10 million stars. Check out the zoomable version for the full experience.
Looking at an image like this is always a bit of a brain-bender because a) 10 million is a huge number and b) the stars are so tightly packed into that image and yet c) that image shows just one tiny bit of our galactic center, d) our entire galaxy contains so many more stars than this (100-400 billion), and e) the Universe perhaps contains as many as 2 trillion galaxies. And if I’m remembering my college math correctly, 400 billion × 2 trillion = a metric crapload of stars. (via bad astronomy)
A spin studio (aka an indoor gym with stationary bikes) in Hamilton, Ontario is dealing with an outbreak of Covid-19 stemming from one asymptomatic patron that has resulted in 69 positive cases so far, even though the studio “followed the rules”. From the CNN report:
SPINCO, in Hamilton, Ontario, just reopened in July and had all of the right protocols in place, including screening of staff and attendees, tracking all those in attendance at each class, masking before and after classes, laundering towels and cleaning the rooms within 30 minutes of a complete class, said Dr. Elizabeth Richardson, Hamilton’s medical officer of health, in a statement.
As the Washington Post reports, patrons were allowed to take their masks off while exercising:
Although Hamilton requires masks to be worn in most public settings, the law includes an exemption for anyone “actively engaged in an athletic or fitness activity.” In keeping with that policy, the studio, SPINCO, allowed riders to remove their masks once clipped into their bikes, and told them to cover up again before dismounting.
The problem here is that while the studio may have followed the rules, they were not the right rules. This outbreak appears to be another clear-cut instance of Covid-19 spread by aerosols. A group of people indoors, without masks, breathing heavily, over long periods of time in what I’m guessing is not a properly ventilated room — this is exactly the sort of thing that has been shown over and over again to be problematic.1 The science is there, but governments and public health agencies have not caught up with this yet. If you take the transmission by aerosols into account, the rules for gyms (and bars and restaurants) being open is that they should probably not be open at all — or if they are, they should be well-ventilated and the wearing of masks should be mandatory at all times.2 (via @DrEricDing)
We’re all so goddamned tired of this fucking pandemic and so people are looking at the development and distribution of a vaccine as the thing that’s going to get us out of this (and quick). But realistically, that’s not what’s going to happen. Carl Zimmer wrote about some of the challenges with Covid-19 vaccines.
The first vaccines may provide only moderate protection, low enough to make it prudent to keep wearing a mask. By next spring or summer, there may be several of these so-so vaccines, without a clear sense of how to choose from among them. Because of this array of options, makers of a superior vaccine in early stages of development may struggle to finish clinical testing. And some vaccines may be abruptly withdrawn from the market because they turn out not to be safe.
“It has not yet dawned on hardly anybody the amount of complexity and chaos and confusion that will happen in a few short months,” said Dr. Gregory Poland, the director of the Vaccine Research Group at the Mayo Clinic.
See also Dr. Fauci’s belief that our best case scenario for returning to something close to normal life in the US is late 2021.
On Twitter, Zimmer also commented on something that I hadn’t really thought about: that all of these vaccines in development in the US are only for adults:
I wrote last month that no trials for kids had started. Update: still no US trials for kids. The goal of having shots ready for them by fall 2021 may be slipping further away.
From Zimmer’s article on the development of a kids’ vaccine:
Only if researchers discovered no serious side effects would they start testing them in children, often beginning with teenagers, then working their way down to younger ages. Vaccine developers are keenly aware that children are not simply miniature adults. Their biology is different in ways that may affect the way vaccines work. Because their airways are smaller, for example, they can be vulnerable to low levels of inflammation that might be harmless to an adult.
These trials allow vaccine developers to adjust the dose to achieve the best immune protection with the lowest risk of side effects. The doses that adults and children need are sometimes different — children get smaller doses of hepatitis B vaccines, for example, but bigger doses for pertussis.
You probably hate reading these kinds of articles; I know I do. But facing up to the reality of our situation, particularly here in the US where our political leadership has utterly failed in protecting us from this virus, is much better than burying our heads in the sand — that’s just not mentally healthy.
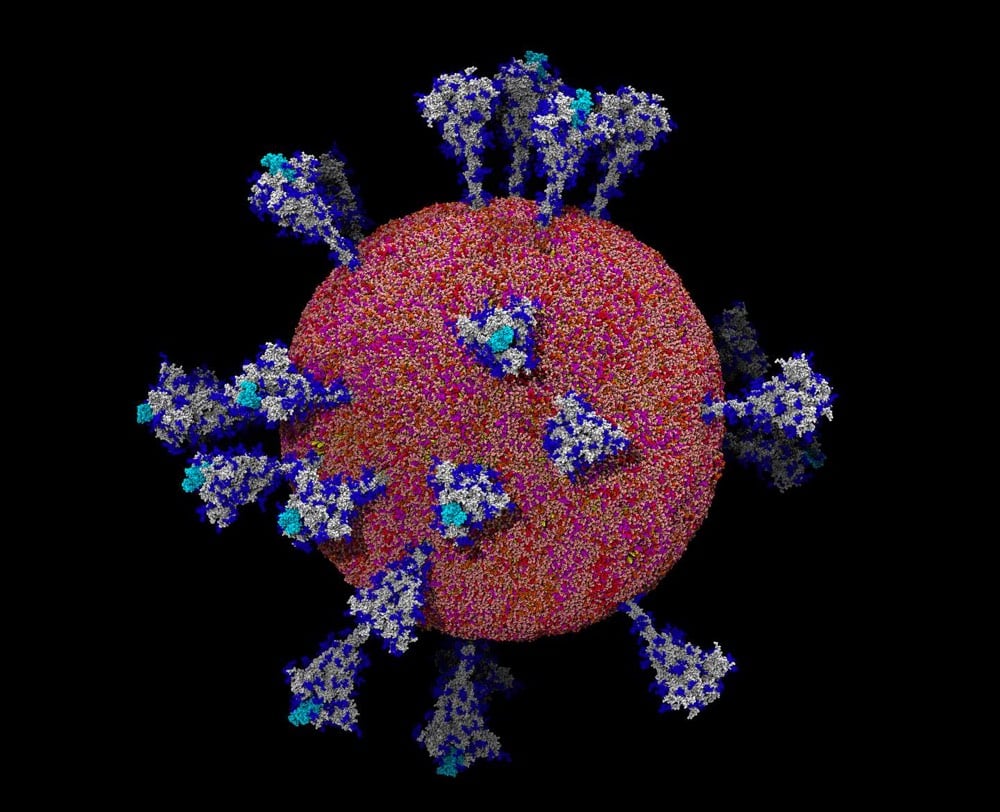
This is a great piece from Carl Zimmer about how much scientists have learned about SARS-CoV-2 through imaging, including how the virus works and prospects for treatment and a vaccine.
Thanks to the work of scientists like Dr. Li, the new coronavirus, known as SARS-CoV-2, is no longer a cipher. They have come to know it in intimate, atomic detail. They’ve discovered how it uses some of its proteins to slip into cells and how its intimately twisted genes commandeer our biochemistry. They’ve observed how some viral proteins throw wrenches into our cellular factories, while others build nurseries for making new viruses. And some researchers are using supercomputers to create complete, virtual viruses that they hope to use to understand how the real viruses have spread with such devastating ease.
I’ve been watching the lectures for MIT’s online Covid-19 class and the thing that has struck me most is just how much scientists have learned about the SARS-CoV-2 virus in such a short amount of time. To be clear, there are many things that they still do not understand about it (and viruses in general), but scientists know this thing upside down and backwards. The depth and breadth of their knowledge is so impressive and I wish more people were aware of it.
In an article that The Atlantic classifies as “politics” rather than “science” or “medicine”, Olga Khazan explores why, more than 8 months into the pandemic, Americans still have little idea about the safety of gathering with others indoors.
For months now, Americans have been told that if we want to socialize, the safest way to do it is outdoors, the better to disperse the droplets that spew from our mouths whenever we do anything but silently purchase grapefruit. But in many parts of the country, this is the last month that the weather will allow people to spend more than a few minutes outside comfortably. And next month, America will celebrate a holiday that is marked by being inside together and eating while talking loudly to old people.
In a nutshell, the lack of federal support/guidance/action is the main reason why people are still so confused about what safety measures to take to reduce their Covid risk:
Still, Ranney says, this [Covid risk] app is the kind of thing the federal government really should have developed by now. It’s odd that in a wealthy, industrialized country, a random researcher is the one designing a tool to keep citizens safe from public-health threats, using data she scraped from a newspaper.
One thing that Khazan doesn’t really get into is the whole aerosols thing, which in my mind is something that most people are still not familiar with, many local & state governments are not taking into account w/r/t recommended safety measures, and requires different risk guidance about the safety of the indoors than if we were just dealing with fomites & droplets. Again, from the excellent Time magazine piece by aerosol chemist Jose-Luis Jimenez:
When it comes to COVID-19, the evidence overwhelmingly supports aerosol transmission, and there are no strong arguments against it. For example, contact tracing has found that much COVID-19 transmission occurs in close proximity, but that many people who share the same home with an infected person do not get the disease. To understand why, it is useful to use cigarette or vaping smoke (which is also an aerosol) as an analog. Imagine sharing a home with a smoker: if you stood close to the smoker while talking, you would inhale a great deal of smoke. Replace the smoke with virus-containing aerosols, which behave very similarly, and the impact is similar: the closer you are to someone releasing virus-carrying aerosols, the more likely you are to breathe in larger amounts of virus. We know from detailed, rigorous studies that when individuals talk in close proximity, aerosols dominate transmission and droplets are nearly negligible.
If you are standing on the other side of the room, you would inhale significantly less smoke. But in a poorly ventilated room, the smoke will accumulate, and people in the room may end up inhaling a lot of smoke over time. Talking, and especially singing and shouting increase aerosol exhalation by factors of 10 and 50, respectively. Indeed, we are finding that outbreaks often occur when people gather in crowded, insufficiently ventilated indoor spaces, such as singing at karaoke parties, cheering at clubs, having conversations in bars, and exercising in gyms. Superspreading events, where one person infects many, occur almost exclusively in indoor locations and are driving the pandemic. These observations are easily explained by aerosols, and are very difficult or impossible to explain by droplets or fomites.
The science is there — it’s the lack of connection between scientists, public health experts & officials, and the government that continues to be a problem.
A few weeks ago during the Q&A session after his lecture for MIT’s online biology class about the pandemic, Dr. Anthony Fauci shared his expert opinion on when things might return to “normal” in the US. Here was my paraphrased tweet about it:
With a very effective vaccine ready in Nov/Dec, distributed widely, and if lots of people take it (i.e. the best case scenario), the earliest we could return to “normal life” in the world is the end of 2021.
At the New Yorker Festival earlier in the week, Michael Specter asked him about a return to normalcy and Fauci elaborated a bit more on this timeline (starts ~10:22 in the video).
When are we gonna get back to something that closely resembles, or is in fact, normal as we knew it?
We’re already making doses, tens and hundreds of millions of doses to be ready, first at least, in graded numbers at the end of the year in November/December. By the time we get to April, we likely will have doses to be able to vaccinate anybody who needs to be vaccinated. But logistically by the time you get everybody vaccinated, it likely will not be until the third or even the beginning of the fourth quarter of 2021.
So let’s say we get a 70% effective vaccine, which I hope we will get, but only 60% of the people get vaccinated. There are going to be a lot of vulnerable people out there, which means that the vaccine will greatly help us to pull back a bit on the restrictions that we have now to maintain good public health, but it’s not going to eliminate things like mask wearing and avoiding crowds and things like that.
So I think we can approach normality, but I don’t think we’re going to be back to normal until the end of 2021. We may do better than that; I hope so but I don’t think so.
Leaving aside what “normal” might mean and who it actually applies to,1 there’s some good news and bad news in there. The good news is, they’re already producing doses of the vaccine to be ready if and when the phase 3 trials are successful. Ramping up production before the trials conclude isn’t usually done because it’s a waste of money if the trials fail, but these vaccines are so critical to saving lives that they’re spending that money to save time. That’s great news.
The bad news is that we’re not even halfway through the pandemic in the best case scenario. We’re going to be wearing masks in public for at least another year (and probably longer than that). Large gatherings of people (especially indoors) will continue to be problematic — you know: movie theaters, concerts, clubs, bars, restaurants, schools, and churches — and folks staying within small pods of trusted folks will likely be the safest course of action.
A change in national leadership in both the executive branch and Senate could change the outlook for the better. We could get some normalcy back even without a vaccine through measures like a national mask mandate/distribution, a real national testing & tracing effort, taking aerosol transmission seriously, and easing the economic pressure to “open back up” prematurely. We’re never going to do as well as Vietnam or Taiwan, but I’d settle for Greece or Norway.
Update: In an interview posted yesterday, Johns Hopkins epidemiologist Dr. Caitlin Rivers gives her best guess at a return to normalcy:
Topol: When do you think we’ll see pre-COVID life restored?
Rivers: I wish I knew. I’m thinking toward the end of 2021. It’s really hard to say with any certainty. We should all be mentally prepared to have quite a bit ahead of us.
Back in June, in a post called Jesus Christ, Just Wear a Face Mask!, I presented a bunch of evidence and arguments for wearing face masks to prevent the spread of Covid-19. Even then it was pretty clear that masks were working. In piece published by Nature yesterday, Lynne Peeples summarizes what the data and science currently says about the effectiveness of wearing face masks. Here is her one-sentence summary:
To be clear, the science supports using masks, with recent studies suggesting that they could save lives in different ways: research shows that they cut down the chances of both transmitting and catching the coronavirus, and some studies hint that masks might reduce the severity of infection if people do contract the disease.
And importantly, even ardently pro-mask scientists agree that masks should be worn in conjunction with taking other precautions: limiting large gatherings, maintaining distance, limiting the time you spend indoors with others, etc.
Now streaming on Netflix, David Attenborough: A Life on Our Planet, a documentary about the 94-year-old broadcaster, naturalist, and international treasure.
In this unique feature documentary, titled David Attenborough: A Life On Our Planet, the celebrated naturalist reflects upon both the defining moments of his lifetime and the devastating changes he has seen. Coming to Netflix October 4 2020, the film addresses some of the biggest challenges facing life on our planet, providing a snapshot of global nature loss in a single lifetime. With it comes a powerful message of hope for future generations as Attenborough reveals the solutions to help save our planet from disaster.
In the trailer (embedded above), Attenborough says “I had the most extraordinary life. It’s only now that I appreciate how extraordinary.” In saying that, he’s speaking not only as a living legend whose long career in television and science has brought him nearly universal acclaim, but also as someone who can look back and see how recognizably and thoroughly the Earth has changed during his lifetime. The depletion of animal populations, the changing climate, the shifting habitats — he’s witnessed firsthand how much humans have fucked up the planet. We should listen to his testimony and suggestions for fixing what he calls “our greatest mistake”. I hope it’s not too late.
A recent study that looked at the brain patterns of crows when performing tasks found evidence that they “know what they know and can ponder the content of their own minds”, an attribute that was previously thought to exist only in humans and some monkeys.
The birds were aware of what they subjectively perceived, flash or no flash, correctly reporting what their sensory neurons recorded, Nieder told STAT. “I think it demonstrates convincingly that crows and probably other advanced birds have sensory awareness, in the sense that they have specific subjective experiences that they can communicate,” he said. “Besides crows, this kind of neurobiological evidence for sensory consciousness only exists in humans and macaque monkeys.”
(via kottke ride home)
In secrecy over the past several months, filmmaker Alex Gibney has been making a documentary film about the US government’s response to the Covid-19 pandemic called Totally Under Control. He and co-directors Ophelia Harutyunyan and Suzanne Hillinger interviewed “countless scientists, medical professionals, and government officials on the inside” to produce the film.
Academy Award-winning filmmaker Alex Gibney, directing with Ophelia Harutyunyan and Suzanne Hillinger, interrogates this question and its devastating implications in Totally Under Control. With damning testimony from public health officials and hard investigative reporting, Gibney exposes a system-wide collapse caused by a profound dereliction of Presidential leadership.
Gibney previously directed Enron: The Smartest Guys in the Room, Going Clear, and Zero Days (all excellent documentaries). The film comes out in theaters on October 13 and on Hulu on October 20.
A group of scientists who believe that WHO and the CDC are being too slow in acknowledging the role of aerosol transmission in spreading Covid-19 have written up a Google Doc of advice for the public: FAQs on Protecting Yourself from COVID-19 Aerosol Transmission.
The goal of these FAQs is to provide information to the general public in an efficient manner about how to prevent aerosol transmission of COVID-19, with the hope that this will allow more informed decision making by individuals or organizations. All of this information has been posted in Twitter and other forums, but can be difficult to find. Having multiple experts working together, and having the ability to update this information also improves its quality. These FAQs represent our best understanding at this time, and should always be similar or more stringent than information provided by CDC, WHO, and most regional & local health authorities. If your authority has a more stringent guideline than discussed here, follow that more stringent guideline.
The group was organized by chemist Jose-Luis Jimenez, who has been studying aerosols for 20 years. You may remember Jimenez from his excellent piece in Time magazine, where he used the analogy of smoke to explain aerosol transmission. Here’s a snippet from the FAQ, highlighting something I’ve been concerned about lately: people wearing face shields instead of masks and employees in stores not wearing masks behind plexiglass shields:
7.13. Are face shields and masks interchangeable?
No, face shields do not offer much protection against aerosols (also see this video), while masks do. Face shields are good for blocking ballistic droplets released by the wearer or that might fly into the wearer’s face when close to others. Face shields are considered a supplement to masks for partial eye protection (but less useful than closed glasses, as discussed above), but not a substitute for them.
7.14. Are plexiglass barriers helpful?
Plexiglass barriers are generally useful to avoid direct droplet infection and direct aerosol transmission whenever people are in close proximity and distance cannot be kept. Therefore, it is recommended to use them as a direct transmission suppression tool at such places, such as a supermarket checkout.
However, as aerosols follow the air movements indoors, the protective effects of the plexiglas barriers against aerosols will be limited. Plexiglas barriers alone are not a sufficient approach to protect against aerosol transmission. Their installation alone cannot protect against indoor aerosol transmission and should not be regarded as safe and sufficient protection.
MIT Technology Review’s Charlotte Jee interviewed Jimenez about the FAQ document.
We update the document all the time. We’re effectively having to be a little WHO or CDC. We’re saying the things that they should be saying. This is frustrating, but it’s the situation we find ourselves in. These organizations have been flat-out refusing to consider if aerosol transmission is important, which leaves people unprotected. So we feel it’s our duty to communicate directly with the public.
Right now, in my opinion as someone who has done a ton of reading about Covid-19, the most best accessible information on how individuals and societies can protect themselves and others during the pandemic (and why) is available in Jimenez’s Time article, Aaron Carroll’s NY Times piece about how to think about risk management, Zeynep Tufekci’s piece in the Atlantic about dispersion and superspreading, and now this Google Doc by Jimenez et al.
Zeynep Tufekci says that we are paying too much attention to the R value of SARS-CoV-2 (basically the measure of its contagiousness) and not nearly enough attention to the k value (“whether a virus spreads in a steady manner or in big bursts, whereby one person infects many, all at once”).
There are COVID-19 incidents in which a single person likely infected 80 percent or more of the people in the room in just a few hours. But, at other times, COVID-19 can be surprisingly much less contagious. Overdispersion and super-spreading of this virus is found in research across the globe. A growing number of studies estimate that a majority of infected people may not infect a single other person. A recent paper found that in Hong Kong, which had extensive testing and contact tracing, about 19 percent of cases were responsible for 80 percent of transmission, while 69 percent of cases did not infect another person. This finding is not rare: Multiple studies from the beginning have suggested that as few as 10 to 20 percent of infected people may be responsible for as much as 80 to 90 percent of transmission, and that many people barely transmit it.
We’ve known, or at least suspected, this about SARS-CoV-2 for awhile now — I linked to two articles about superspreading back in May and June — but Tufekci says we have not adjusted our thinking about what that means for prevention. We should be avoiding superspreading environments/events (“Avoid Crowding, Indoors, low Ventilation, Close proximity, long Duration, Unmasked, Talking/singing/Yelling”), doing backwards contact tracing, and rapid testing.
In an overdispersed regime, identifying transmission events (someone infected someone else) is more important than identifying infected individuals. Consider an infected person and their 20 forward contacts-people they met since they got infected. Let’s say we test 10 of them with a cheap, rapid test and get our results back in an hour or two. This isn’t a great way to determine exactly who is sick out of that 10, because our test will miss some positives, but that’s fine for our purposes. If everyone is negative, we can act as if nobody is infected, because the test is pretty good at finding negatives. However, the moment we find a few transmissions, we know we may have a super-spreader event, and we can tell all 20 people to assume they are positive and to self-isolate-if there is one or two transmissions, it’s likely there’s more exactly because of the clustering behavior. Depending on age and other factors, we can test those people individually using PCR tests, which can pinpoint who is infected, or ask them all to wait it out.
Part of the problem is that dispersion and its effects aren’t all that intuitive.
Overdispersion makes it harder for us to absorb lessons from the world because it interferes with how we ordinarily think about cause and effect. For example, it means that events that result in spreading and non-spreading of the virus are asymmetric in their ability to inform us. Take the highly publicized case in Springfield, Missouri, in which two infected hairstylists, both of whom wore masks, continued to work with clients while symptomatic. It turns out that no apparent infections were found among the 139 exposed clients (67 were directly tested; the rest did not report getting sick). While there is a lot of evidence that masks are crucial in dampening transmission, that event alone wouldn’t tell us if masks work. In contrast, studying transmission, the rarer event, can be quite informative. Had those two hairstylists transmitted the virus to large numbers of people despite everyone wearing masks, it would be important evidence that, perhaps, masks aren’t useful in preventing super-spreading.
The piece is an important read and interesting throughout: just read the whole thing.
For Kurzgesagt’s latest video, they explore the challenges the world faces in attempting to get the rate of climate change under control before it’s too late and how to get there.
Climate change is just too much. There is never any good news. Only graphs that get more and more red and angry. Almost every year breaks some horrible record, from the harshest heat waves to the most rapid glacier melt. It’s endless and relentless.
We have known for decades that rapid climate change is being caused by the release of greenhouse gases. But instead of reducing them, in 2019 the world was emitting 50% more CO2 than in the year 2000. And emissions are still rising. Why is that? Why is it so hard to just stop emitting these gases?
According to the video, global population growth and economic growth will be working against us over the next few decades and that increasing our energy efficiency and lowering emissions from energy sources are the main ways in which we will be able to slow things down. It’s worth noting that on the wizard vs. prophet continuum, this video is firmly in the wizard camp. That’s not wrong or bad; it’s just that other people have different ideas about how to combat climate change.
Newer posts
Older posts
Socials & More