kottke.org posts about medicine
According to an ongoing investigation at The Atlantic, the US has tested only about 14,000 people for COVID-19 so far (a stat CDC data seems to confirm). 14,000 out of 330 million people. Olga Khazan writes about the four main reasons why the US is so behind in testing for the virus.
Interviews with laboratory directors and public-health experts reveal a Fyre-Festival-like cascade of problems that have led to a dearth of tests at a time when America desperately needs them. The issues began with onerous requirements for the labs that make the tests, continued because of arcane hurdles that prevented researchers from getting the right supplies, and extended to a White House that seemed to lack cohesion in the pandemic’s early days. Getting out lots of tests for a new disease is a major logistical and scientific challenge, but it can be pulled off with the help of highly efficient, effective government leadership. In this case, such leadership didn’t appear to exist.
Here’s another take on the problem from a few days ago in the NY Times.
The US has bungled the situation so badly that a pair of Chinese foundations announced this morning that they were donating 500,000 testing kits and 1 million masks to the US. Last month in my Asian travelogue, I wrote that my main observation after spending three weeks in Asia was: “America is a rich country that feels like a poor country”. That we have to rely on foreign aid in situations like this is a good example of what I was referring to.
The number one recommendation on the list of protective measures for COVID-19 from both WHO and the CDC is to regularly wash your hands. The CDC in particular recommends hand-washing over using hand sanitizer.
Vox recently talked with chemistry professor Palli Thordarson about why washing with soap is so effective when dealing with coronaviruses.
The soap takes care of the virus much like it takes care of the oil in the water. “It’s almost like a crowbar; it starts to pull all the things apart,” Thordarson says.
One side of the soap molecule (the one that’s attracted to fat and repelled by water) buries its way into the virus’s fat and protein shell. Fortunately, the chemical bonds holding the virus together aren’t very strong, so this intrusion is enough to break the virus’s coat. “You pull the virus apart, you make it soluble in water, and it disintegrates,” he says.
Then the harmless shards of virus get flushed down the drain. (And even if it the soap doesn’t destroy every virus, you’ll still rid them from your hands with soap and water, as well as any grease they may be clinging to.)
And why do you need to wash for 20 seconds? Because that gives soap time to do its work.
First off, your skin is wrinkly, and it takes time for soap to penetrate into all the tiny folds and demolish the viruses that lurk within. Then the soap needs a few moments to do its chemical work. “You do need a bit of time for all the soap to interact back and forth with the virus particle,” he says. Twenty seconds should do the trick just fine.
See also Why Soap Works from the NY Times, which explains why soap & water is better than hand sanitizer in these cases:
On the whole, hand sanitizers are not as reliable as soap. Sanitizers with at least 60 percent ethanol do act similarly, defeating bacteria and viruses by destabilizing their lipid membranes. But they cannot easily remove microorganisms from the skin. There are also viruses that do not depend on lipid membranes to infect cells, as well as bacteria that protect their delicate membranes with sturdy shields of protein and sugar. Examples include bacteria that can cause meningitis, pneumonia, diarrhea and skin infections, as well as the hepatitis A virus, poliovirus, rhinoviruses and adenoviruses (frequent causes of the common cold).
Update: Thordarson also wrote an article for The Guardian on how effective soap is at killing coronavirus.
Many stores have long since sold out of hand sanitizer in the US and washing your hands is a better move anyway, but if you’d like to have some sanitizer on hand for when you can’t get to a sink, the World Health Organization has you covered. The WHO recipe is for making 10-liter batchs, so Popular Science helpfully scaled it down to a more reasonable size:
1 cup 99% isopropyl alcohol
1 tablespoon 3% hydrogen peroxide
1 teaspoon 98% glycerin/glycerol
1/4 cup, 1 tablespoon, and 1 teaspoon sterile distilled or boiled cold water
To the alcohol, add the hydrogen peroxide & glycerin and stir or shake if you’re mixing in a container with a lid. Then add the water.
For COVID-19 prevention, the CDC recommends a hand sanitizer that contains at least 60% alcohol; this recipe will end up being about 75% alcohol. The Popular Science piece also includes another recipe for a hand sanitizing gel that’s much closer to store-bought gels that involves mixing isopropyl alcohol, aloe vera gel, and tea tree oil. They also note that vodka does not contain enough alcohol to meet the CDC’s recommendation, especially when mixed with the other ingredients.
In recent years, many media outlets have joined publications like the WSJ and NY Times in erecting paywalls around their online offerings, giving visitors access to a few articles a month before asking them to pay for unlimited access. Due to the continuing worldwide COVID-19/coronavirus crisis and in order to make information about the pandemic more accessible to the public, several publications have dropped their paywalls for at least some of their coronavirus coverage (thanks to everyone who responded to my tweet about this).
Among them are The Atlantic, WSJ, Talking Points Memo, Globe and Mail, Seattle Times, Miami Herald (and other McClatchy-owned properties), Toronto Star, Stat, Dallas Morning News, Medium, NY Times, Washington Post, Baltimore Sun, Chicago Tribune, Christian Science Monitor and several medical/science journals. Notably, The Guardian relies on online subscription revenue but doesn’t put anything behind a paywall, including their coronavirus coverage.
In addition, a group of archivists have created an online directory of scientific papers related to coronaviruses, available for free download.
“These articles were always written to be shared with as many people as possible,” Reddit user “shrine,” an organizer of the archive, said in a call. “From every angle that you look at it, [paywalled research] is an immoral situation, and it’s an ongoing tragedy.”
Kudos to those media organizations for doing the right thing — this information can save people’s lives. Let’s hope others (*cough* Washington Post) will soon follow suit. And if you find the coverage helpful, subscribe to these outlets!
BTW, like The Guardian, kottke.org is supported by readers just like you who contribute to make sure that every single thing on the site is accessible to everyone. If you’re a regular reader, please consider supporting this experiment in openness.
Update: Added the NY Times to the list above. I am also hearing that many European papers are not dropping their paywalls in the face of the crisis.
Update: Added several media outlets to the list, including Washington Post and Chicago Tribune. At this point, it seems to be standard practice now (at least in the US & Canada) so this will be the final update. (thx, @maschweisguth)
In a media briefing that’s still ongoing as I’m writing this, Dr. Tedros Adhanom Ghebreyesus, the Director General of the World Health Organization, has officially characterized the COVID-19 outbreak as a pandemic. A pandemic is defined as:
An influenza pandemic is a global epidemic caused by a new influenza virus to which there is little or no pre-existing immunity in the human population. Influenza pandemics are impossible to predict; and they may be mild, or cause severe disease or death. Severe disease may occur in certain risk groups, which may correspond to those at risk of severe disease due to seasonal influenza.
Here’s a transcript of Dr. Tedros’s opening remarks from the briefing.
WHO has been assessing this outbreak around the clock and we are deeply concerned both by the alarming levels of spread and severity, and by the alarming levels of inaction.
We have therefore made the assessment that COVID-19 can be characterized as a pandemic.
Pandemic is not a word to use lightly or carelessly. It is a word that, if misused, can cause unreasonable fear, or unjustified acceptance that the fight is over, leading to unnecessary suffering and death.
Describing the situation as a pandemic does not change WHO’s assessment of the threat posed by this virus. It doesn’t change what WHO is doing, and it doesn’t change what countries should do.
Progress on fighting COVID-19 can be made everywhere when the right steps are taken:
If countries detect, test, treat, isolate, trace, and mobilize their people in the response, those with a handful of cases can prevent those cases becoming clusters, and those clusters becoming community transmission.
Even those countries with community transmission or large clusters can turn the tide on this virus.
Several countries have demonstrated that this virus can be suppressed and controlled.
The challenge for many countries who are now dealing with large clusters or community transmission is not whether they can do the same — it’s whether they will.
But WHO also acknowledges how disruptive the pandemic can be:
We are grateful for the measures being taken in Iran, Italy and the Republic of Korea to slow the virus and control their epidemics.
We know that these measures are taking a heavy toll on societies and economies, just as they did in China.
All countries must strike a fine balance between protecting health, minimizing economic and social disruption, and respecting human rights.
And in closing he deflects attention from the word “pandemic”:
Let me give you some other words that matter much more, and that are much more actionable.
Prevention.
Preparedness.
Public health.
Political leadership.
And most of all, people.
We’re in this together, to do the right things with calm and protect the citizens of the world. It’s doable.
Yascha Mounk writing for The Atlantic:
These three facts imply a simple conclusion. The coronavirus could spread with frightening rapidity, overburdening our health-care system and claiming lives, until we adopt serious forms of social distancing.
This suggests that anyone in a position of power or authority, instead of downplaying the dangers of the coronavirus, should ask people to stay away from public places, cancel big gatherings, and restrict most forms of nonessential travel.
Given that most forms of social distancing will be useless if sick people cannot get treated-or afford to stay away from work when they are sick-the federal government should also take some additional steps to improve public health. It should take on the costs of medical treatment for the coronavirus, grant paid sick leave to stricken workers, promise not to deport undocumented immigrants who seek medical help, and invest in a rapid expansion of ICU facilities.
This is very close to my own personal thinking right now, particularly after watching this excellent video about exponential growth and epidemics.
From 3blue1brown’s Grant Sanderson, this is an excellent quick explanation of exponential growth and how we should think about it in relation to epidemics like COVID-19. Depending on how rusty your high school math is, you might need to rewind a couple of times to fully grasp the explanation, but you should persevere and watch the whole thing.
The most important bit is at the end, right around the 7:45 mark, when he talks about how limiting person-to-person exposure and decreasing the probability of exposures becoming infections can have a huge effect on the total number of people infected because the growth is exponential. If large numbers of people start doing things like limiting travel, cancelling large gatherings, social distancing, and washing their hands frequently, the total number of infections could fall by several orders of magnitude, making the exponential work for us, not against us. Small efforts have huge results. If, as in the video, you’re talking about 100 million infected in two months (at the current transmission rate) vs. 400,000 (at the lowered rate) and if the death rate of COVID-19 is between 1-3%, you’re looking at 1-3 million dead vs. 4-12,000 dead.
So let’s start flattening that exponential curve. South Korea and China both seem to have done it, so there’s no reason the rest of the world can’t through aggressive action. (thx, david)
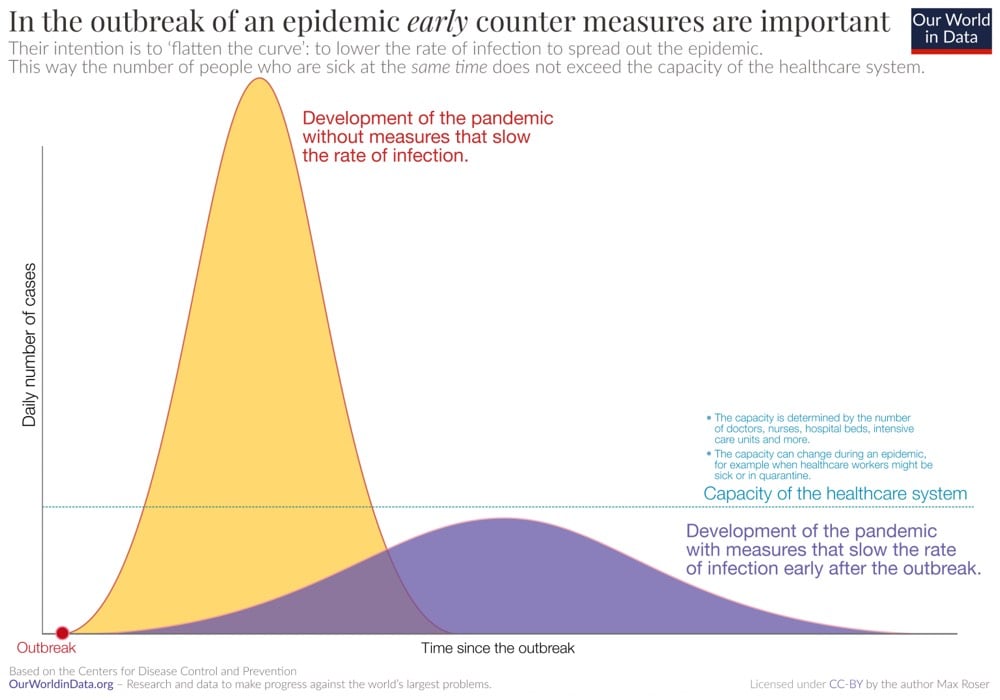
Update: Vox has a nice explainer on what epidemiologists refer to as “flattening the curve”.
Yet the speed at which the outbreak plays out matters hugely for its consequences. What epidemiologists fear most is the health care system becoming overwhelmed by a sudden explosion of illness that requires more people to be hospitalized than it can handle. In that scenario, more people will die because there won’t be enough hospital beds or ventilators to keep them alive.
A disastrous inundation of hospitals can likely be averted with protective measures we’re now seeing more of — closing schools, canceling mass gatherings, working from home, self-quarantine, avoiding crowds - to keep the virus from spreading fast.
Epidemiologists call this strategy of preventing a huge spike in cases “flattening the curve”.
Here’s the relevant graphic explanation from Our World in Data’s COVID-19 package:
A few days ago, Dr. Daniele Macchini, a physician in Bergamo, Italy, made a long post on Facebook (also reprinted here) about how the outbreak of COVID-19 (coronavirus) is overwhelming the hospitals there and pleads with the rest of the world to take the virus seriously. The original post is in Italian and Google Translate does pretty well with it. Dr. Silva Stringhini translated the important bits of Dr. Macchini’s post in this Twitter thread and is somewhat easier to read:
After much thought about whether and what to write about what is happening to us, I felt that silence was not responsible.
“I will therefore try to convey to people far from our reality what we are living in Bergamo in these days of Covid-19 pandemic. I understand the need not to create panic, but when the message of the dangerousness of what is happening does not reach people I shudder.
“I myself watched with some amazement the reorganization of the entire hospital in the past week, when our current enemy was still in the shadows: the wards slowly ‘emptied’, elective activities were interrupted, intensive care were freed up to create as many beds as possible.
“All this rapid transformation brought an atmosphere of silence and surreal emptiness to the corridors of the hospital that we did not yet understand, waiting for a war that was yet to begin and that many (including me) were not so sure would ever come with such ferocity.
“I still remember my night call a week ago when I was waiting for the results of a swab. When I think about it, my anxiety over one possible case seems almost ridiculous and unjustified, now that I’ve seen what’s happening. Well, the situation now is dramatic to say the least.
“The war has literally exploded and battles are uninterrupted day and night. But now that need for beds has arrived in all its drama. One after the other the departments that had been emptied fill up at an impressive pace.
“The boards with the names of the patients, of different colours depending on the operating unit, are now all red and instead of surgery you see the diagnosis, which is always the damned same: bilateral interstitial pneumonia.
Dr. Macchini urges: “Let’s stop saying it’s a bad flu.” But this is the part that stopped me in my tracks and got me to write this post:
So have patience, too, that you cannot go to the theater, museums or gym. Try to have mercy on that myriad of older people you could exterminate.
His overall message is that we shouldn’t panic, but that we should take COVID-19 seriously. The goal here is to keep the most vulnerable of us as safe as possible and work to slow the spread of the virus so it doesn’t overwhelm our healthcare system. So let’s do that — the elderly and those most at risk are counting on us.
There are certain links I’ve posted here that I think about more often than others. One that I think a lot about — weekly at least — is Emma Young’s story for Mosaic about Iceland’s very successful program that’s steered the nation’s teens away from drug and alcohol abuse. At the center of the Icelandic strategy is an insight by psychologist Harvey Milkman about a strategy of replacing substance and other unhealthy addictions with healthier natural highs:
At Metropolitan State College of Denver, Milkman was instrumental in developing the idea that people were getting addicted to changes in brain chemistry. Kids who were “active confronters” were after a rush — they’d get it by stealing hubcaps and radios and later cars, or through stimulant drugs. Alcohol also alters brain chemistry, of course. It’s a sedative but it sedates the brain’s control first, which can remove inhibitions and, in limited doses, reduce anxiety.
“People can get addicted to drink, cars, money, sex, calories, cocaine — whatever,” says Milkman. “The idea of behavioural addiction became our trademark.”
This idea spawned another: “Why not orchestrate a social movement around natural highs: around people getting high on their own brain chemistry — because it seems obvious to me that people want to change their consciousness — without the deleterious effects of drugs?”
BTW, this is a somewhat controversial view but it has always made sense to me for those with mild addictions or depression. Speaking strictly for myself, I’ve found that when healthier alternatives are available to me (spending time with family & friends, exercise, exploring, reading a good book), I spend a lot less time mindlessly doing things that give me the same sort of brain buzz but which I don’t consider positive or worthwhile (drinking alcohol, watching TV, eating poorly, and especially reloading Instagram over and over again like a lab rat slapping that lever to get more cocaine).
But back to Iceland. By giving teens access to more healthy activities, getting parents more involved in their children’s lives, implementing curfews, and administering annual surveys, the country has made great strides over the past two decades:
Today, Iceland tops the European table for the cleanest-living teens. The percentage of 15- and 16-year-olds who had been drunk in the previous month plummeted from 42 per cent in 1998 to 5 per cent in 2016. The percentage who have ever used cannabis is down from 17 per cent to 7 per cent. Those smoking cigarettes every day fell from 23 per cent to just 3 per cent.
The way the country has achieved this turnaround has been both radical and evidence-based, but it has relied a lot on what might be termed enforced common sense. “This is the most remarkably intense and profound study of stress in the lives of teenagers that I have ever seen,” says Milkman. “I’m just so impressed by how well it is working.”
Young did a follow-up last year about the expansion of the program into other areas of the world.
Even though larger animals like elephants and blue whales have up to 100 billion more cells than humans in their bodies — and therefore many more chances for harmful mutations to develop — they are much more immune to cancer. This is called Peto’s paradox the subject of Kurzgesagt’s latest video. Scientists aren’t sure why this happens, but one hypothesis is that in order to have grown so large, the evolutionary process that resulted in these animals provided built-in defenses against cancer that other animals didn’t need. Further reading on the topic is available here.
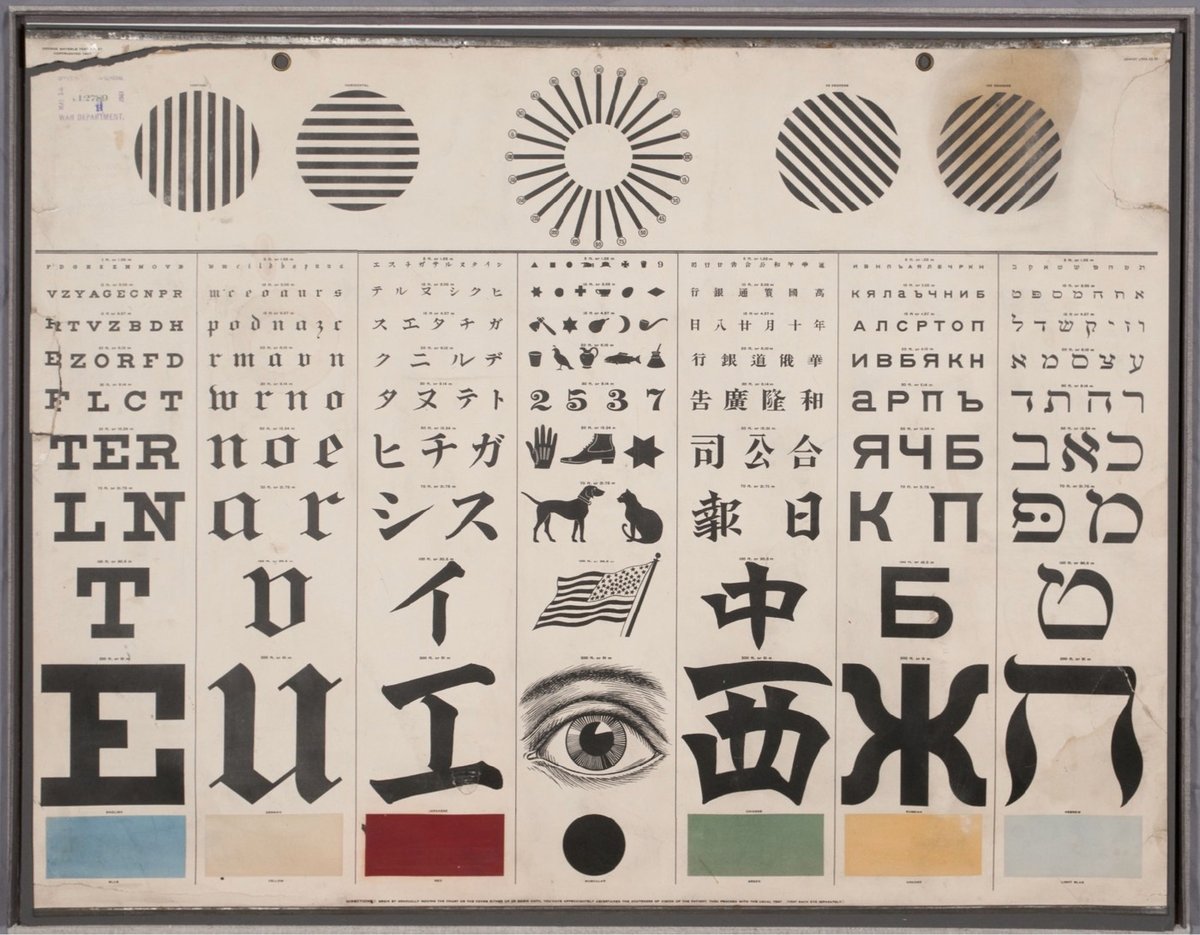
From the collection of the US National Library of Medicine, an eye test chart designed by George Mayerle around 1907 to be a complete vision testing solution for speakers of several languages.
Running through the middle of the chart, the seven vertical panels test for acuity of vision with characters in the Roman alphabet (for English, German, and other European readers) and also in Japanese, Chinese, Russian, and Hebrew. A panel in the center replaces the alphabetic characters with symbols for children and adults who were illiterate or who could not read any of the other writing systems offered. Directly above the center panel is a version of the radiant dial that tests for astigmatism. On either side of that are lines that test the muscular strength of the eyes. Finally, across the bottom, boxes test for color vision, a feature intended especially (according to one advertisement) for those working on railroads and steamboats.
Mayerle was a German optometrist working in San Francisco when he made the chart, designing it for use in a city with a diverse population. My pals at 20x200 are offering limited-edition prints of Mayerle’s chart in a variety of sizes.
See also the history & typography of eye test charts, Optician Sans (a font based on eye chart typography), and Eye Charts for Drones.
This is the most metal shit ever: the doctors removing violinist Dagmar Turner’s brain tumor woke her up during the procedure to play the violin to make sure that she didn’t lose any parts of her brain vital to her playing.
After explaining concerns she had over losing the ability to play the violin, Prof Ashkan and the neurosurgical team at King’s devised a plan. Prior to Dagmar’s operation they spent two hours carefully mapping her brain to identify areas that were active when she played the violin and those responsible for controlling language and movement. They also discussed with Dagmar the idea of waking her mid-procedure so she could play. This would ensure the surgeons did not damage any crucial areas of the brain that controlled Dagmar’s delicate hand movements specifically when playing the instrument. With her agreement, a team of surgeons, anaesthetists and therapists went on to meticulously plan the procedure.
During the operation Prof Ashkan and the team performed a craniotomy (an opening in the skull) and Dagmar was brought round from the anaesthetic. She played violin while her tumour was removed, while closely monitored by the anaesthetists and a therapist.

This site is making N95 respirator masks that work with facial recognition software, so that, for example, you can unlock your phone while still wearing a mask.
After uploading your face, we use computational mapping to convert your facial features into an image printed onto the surface of N95 surgical masks without distortion.
Our printer uses inks made of natural dyes. It’s non-toxic and doesn’t affect breathability.
You can use your mask for everyday life as a barrier for airborne particle droplets.
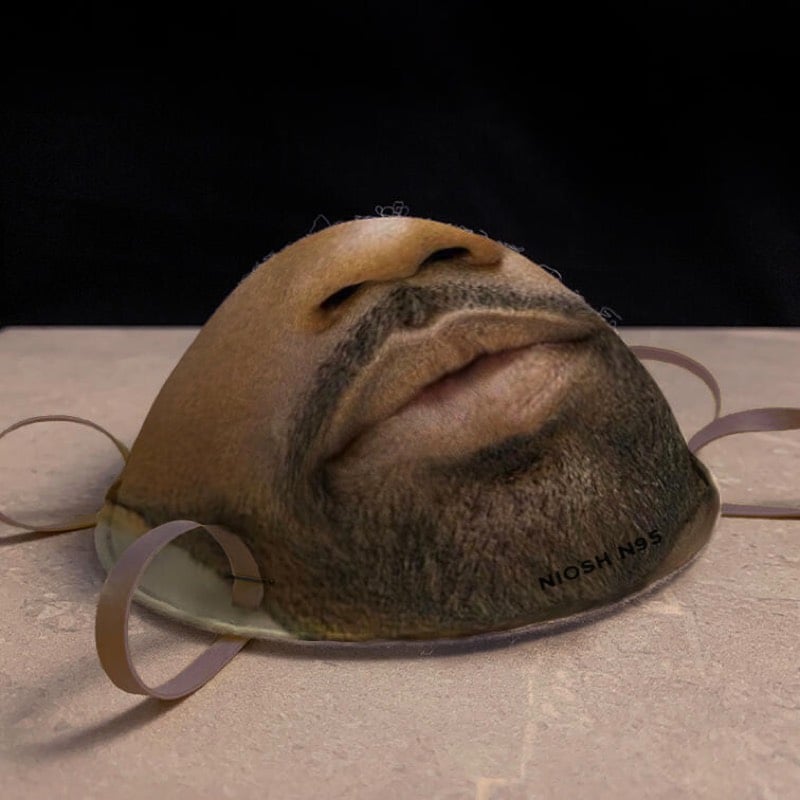
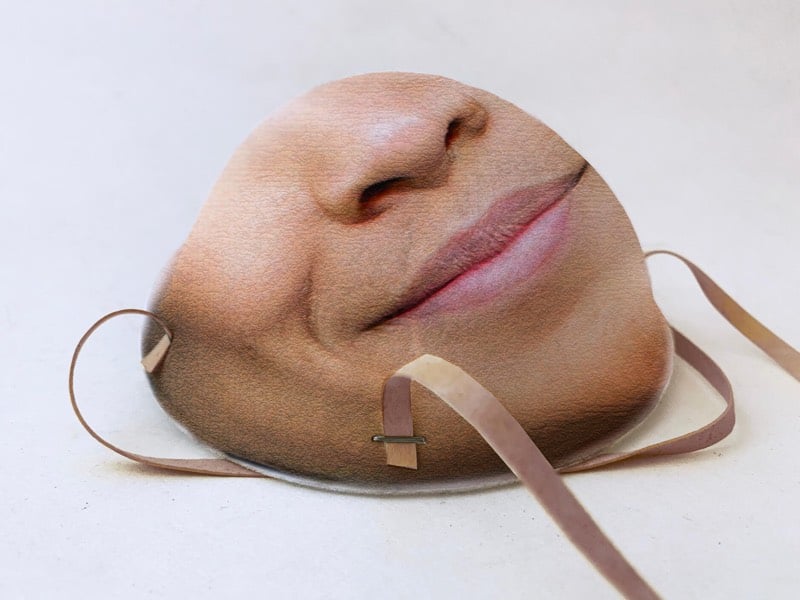
It is unclear whether these will actually ship or not — “Q: Is this a joke? A: Yes. No. We’re not sure.” — but they’re definitely not planning to make them while there are mask shortages related to COVID-19. And it appears the masks will work with iPhones…you just add a new face (while wearing the mask) to your phone’s face database.
With news of more than 70,000 confirmed cases and 1700 deaths from the COVID-19 virus, the importance of handwashing is once again front and center. Using data from a 1978 study on the hygiene of health professionals, this is a map of the most missed areas when washing hands.
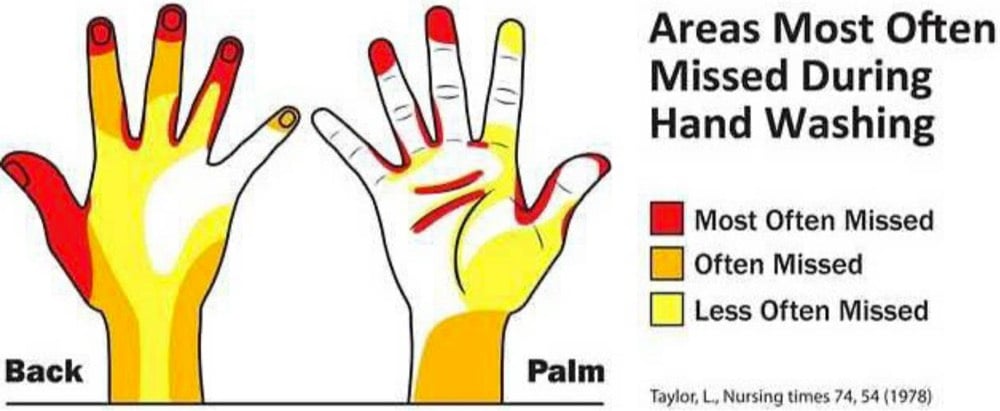
This more recent paper contains a short review of various studies of missed areas, most of which conclude that people often forget to wash their fingertips:
In 2008, the WHO designed a handwashing leaflet, making reference to Taylor, who indicated that the fingertips, interdigital areas, thumbs, and wrists are the most commonly missed areas in handwashing. Pan et al. also found that the tips of the nails and the fingertips had the largest amount of residual florescent stains left after handwashing among healthcare workers in Taiwan. The commonly missed areas among medical students in the study conducted by Vanyolos et al. was the first metacarpal, the proximal part of the palm (lateral), the distal phalanges, and the nail beds. In healthcare workers in Škodová et al.’s study, the thumbs and fingertips were the most commonly missed areas. In this study, the most frequently missed area was also the fingertips. However, the medial aspect and back of the hand were the second and third most missed areas, respectively. Moreover, the interdigital area and the front and back of the fingers were the least missed areas, which is in contrast to Taylor’s study.
So wash those fingertips! Here’s the CDC-recommended guide to washing your hands properly.
- Wet your hands with clean, running water (warm or cold), turn off the tap, and apply soap.
- Lather your hands by rubbing them together with the soap. Lather the backs of your hands, between your fingers, and under your nails.
- Scrub your hands for at least 20 seconds. Need a timer? Hum the “Happy Birthday” song from beginning to end twice.
- Rinse your hands well under clean, running water.
- Dry your hands using a clean towel or air dry them.
See also this TED Talk on how to properly dry your hands with a paper towel. (via a map a day)



For her series One Person City, photographer nicoco has been taking photos of Shanghai that emphasize how deserted the city was due to the COVID-19 outbreak that has killed more than 1000 people in China. In an interview with Hyperallergic, the photographer said:
My objective for this series was to capture the feeling of apocalyptic emptiness. Some of the photos may look as if they were captured at strange early morning hours, but as a collection, it seeks to reinforce there were no people, anywhere.
These are Shanghai’s busiest locations that can compare to Times Square in New York City, Big Ben in London, the Bean in Chicago, or the Washington Monument in DC. They are very popular on an average day, and very, very popular during holidays as domestic tourists and residents spend time with their families and check out festive displays, shop, or just meander around.
You can find the photos on her Instagram.
Shake is a typeface made from the real handwriting of a person living with Parkinson’s disease. Creative director Morten Halvorsen:
My mother was diagnosed with Parkinson’s eight years ago. And her handwriting has changed in the years since. I created this font to preserve her handwriting, and enable her to continue to write with her own letters.
A new version of the font will be available each year to capture his mother’s worsening condition. Donate a few dollars (or more!) to download the font — all proceeds go to finding a cure. You can also download a template so that you can document the handwriting of a loved one living with Parkinson’s — for a fee (donated to Parkinson’s research), Halvorsen will turn it into a font for you. (thx, kevin)
With the Wuhan coronavirus in the news, this is a timely release from Netflix: Pandemic is a 6-part series on the inevitable worldwide disease outbreak and what’s being done to stop it, or at least to mitigate its effects.
At the Sebrell Funeral Home in Ridgeland, MS (just outside of Jackson), they perform funerals and cremations for people with HIV/AIDS, some of whom have been abandoned by their families because of their disease or sexual orientation.
In almost one-third of the AIDS-related deaths serviced by Sebrell Funeral Home, the family or next-of-kin will either abandon the deceased entirely or refuse to accept the cremains.
HIV/AIDS is a growing problem in the American South, due to social stigma, poverty, and decreased access to healthcare. In this short documentary, we meet Trey Sebrell, who thinks of caring for all deceased people, no matter who they were in life, as part of his mission as a funeral director.
In a piece for the NY Times, obstetrician-gynecologist Dr. Lisa Harris shares her experience of a typical day at her practice, where she and her staff provide abortions.
My youngest patient of the day is 14 and here with her parents. The oldest patient is 41, here with her husband. As on all days, my patients come from every walk of life. Most have children already; many have arranged their appointment so that they’ll be done in time to pick them up after school. They assure me, again, that they are certain about their decision.
By the end of the day, I’ve seen 17 people, and made sure each received the care and time she needed. After counseling, two others left without having an abortion. One decided to continue her pregnancy and become a parent. Another appeared to need more time to think about it, and I encouraged her to do that. I support all of my patients’ decisions and needs; doing so is core to my work.
This was a typical day, and on the way home some of it plays back in my mind. A mother of three crosses herself and then takes the mifepristone pill she requested. Another requests a copy of the ultrasound picture for her memory box. After the abortion procedure, one asks to see what had been in her uterus and is relieved that the fetus is less than an inch, so much smaller than she had imagined.
See also What Illegal Abortion Was Like in the 1960s and Harrowing Illegal Abortion Stories from Before Roe v. Wade.
From filmmaker David Freid, Nobody Dies in Longyearbyen is a short film about Longyearbyen, Norway, the one of the northernmost towns in the world. The town of about 2100 residents is situated on the Svalbard archipelago and is the home of the Global Seed Vault. Freid went to investigate the rumor that no one is allowed to die in Longyearbyen and discovered that if climate change results in the permafrost melting in places like this, diseases from long ago may be released back into the world.
But for more than 70 years, not a single person has been buried in Longyearbyen. That’s due to the region’s year-round sub-zero temperatures: Bodies don’t decompose, but are preserved, as if mummified, in the permafrost. Should anyone die there, the government of Svalbard requires that the body is flown or shipped to mainland Norway to be interred.
See also A Trip to the Northernmost Town on Earth.
Ten years ago, in the midst of the 2009 swine flu pandemic, I wrote about the manufacturing process for the H1N1 flu vaccine. It involves billions of chicken eggs.
The most striking feature of the H1N1 flu vaccine manufacturing process is the 1,200,000,000 chicken eggs required to make the 3 billion doses of vaccine that may be required worldwide. There are entire chicken farms in the US and around the world dedicated to producing eggs for the purpose of incubating influenza viruses for use in vaccines. No wonder it takes six months from start to finish.
The post holds up pretty well because, according to the CDC, this is still the way most flu vaccines in America are manufactured. Here’s a look at pharmaceutical company GSK’s egg-based process:
Two other techniques for making flu vaccines were approved for use in the US in 2012 and 2013 respectively, cell-based flu vaccines:
‘Cell-based’ refers to how the flu vaccine is made. Most inactivated influenza vaccines are produced by growing influenza viruses in eggs. The influenza viruses used in the cell-based vaccine are grown in cultured cells of mammalian origin instead of in hens’ eggs.
A cell-based flu vaccine was developed as an alternative to the egg-based manufacturing process. Cell culture technology is potentially more flexible than the traditional technology, which relies upon adequate supply of eggs. In addition, the cell-based flu vaccine that uses cell-based candidate vaccine viruses (CVVs) has the potential to offer better protection than traditional, egg-based flu vaccines as a result of being more similar to flu viruses in circulation.
And recombinant flu vaccines:
NIAID and its industry partners have made progress in moving from both the egg-based and cell-based flu vaccine production methods toward recombinant DNA manufacturing for flu vaccines. This method does not require an egg-grown vaccine virus and does not use chicken eggs at all in the production process. Instead, manufacturers isolate a certain protein from a naturally occurring (“wild type”) recommended flu vaccine virus. These proteins are then combined with portions of another virus that grows well in insect cells. The resulting “recombinant” vaccine virus is then mixed with insect cells and allowed to replicate. The flu surface protein called hemagglutinin is then harvested from these cells and purified.
Both of these new techniques make production quicker, thereby resulting in more effective vaccines because they are more likely to match the strains of whatever’s “going around”.
As a reminder, you should get a flu shot every year in the fall. The CDC recommends that “everyone 6 months of age and older should get a flu vaccine every season with rare exception”, especially those “who are at high risk of serious complications from influenza”. Flu vaccines are covered by your health insurance without copay (thanks, Obama!) and are often available at drug stores without an appointment or a long wait. So go get one!
For the New Yorker, Nick Paumgarten writes about this year’s measles outbreak in the US, the largest such outbreak in decades. The outbreak is solely due to a growing number of people who decline to vaccinate their children, so the fight has become one not against a disease, as it was decades ago, but against dangerous ideas.
But, if we have to pick a Patient Zero, Andrew Wakefield will do. Wakefield is the British gastroenterologist who produced the notorious article, published in The Lancet in 1998, linking the M.M.R. vaccine to autism. The study, which featured just twelve subjects, was debunked, the article was pulled, and Wakefield lost his license to practice medicine — as well as his reputation, in scientific circles anyway. But, owing to his persistence in the years since, his discredited allegations have spread like mold. In the anti-vaxxer pantheon, he is martyr and saint. There are also the movement’s celebrities, such as Jenny McCarthy and Robert F. Kennedy, Jr., stubborn in the face of ridicule, and the lesser-known but perhaps no less pernicious YouTube evangelists, such as Toni Bark, a purveyor of homeopathic products, and the Long Island pediatrician Lawrence Palevsky. If your general practitioner is Dr. Google, you can find a universe of phony expertise. The movement seems to sniff out susceptibility. Not surprisingly, there is money there, though the financial incentives behind this strand of advocacy are less clear than, say, what has led the Koch brothers to champion fossil fuels. This spring, the Washington Post reported that the New York hedge-fund manager Bernard Selz and his wife, Lisa, have given more than three million dollars to anti-vaccination causes and helped finance “Vaxxed,” Wakefield’s 2016 documentary, which purports to reveal a C.D.C. conspiracy to cover up the connection between vaccines and autism. Needless to say, the anti-vaccination ethos is by no means exclusive to the New York tristate-area Orthodox community. It thrives in certain pockets — affluent boho-yoga moms, evangelical Christians, Area 51 insurgents. The vaccination rates are about the same in Monsey and in Malibu. Before New Square, the three most recent big outbreaks of measles occurred among Somali immigrants, in Minnesota; Amish farmers, in Ohio; and a hodgepodge of visitors to Disneyland.
“It’s shocking how strong the anti-vax movement is,” Zucker said. “What surprises me is the really educated people who are passionately against vaccinations. I see this as part of a larger war against science-based reality. We need to study vaccine hesitancy as a disease.” He gave a TEDX talk recently about the crippling disconnect between the speed at which information, good or bad, spreads now and the slow, grinding pace of public-health work. He managed, by way of the general theory of relativity, to establish the equivalence of H1N1, Chewbacca Mask Lady, and Pizzagate: “How do we immunize and protect ourselves from the damaging effects of virality?”
The internet is such an efficient way to spread ideas (regardless of their validity) that you begin to wonder if instant global individual-to-individual and individual-to-everyone communication is an insurmountable Great Filter for societies.
The servers at The Restaurant of Mistaken Orders, a series of pop-up restaurants in Tokyo, are all living with dementia, which means that you might not receive what you ordered.
All of our servers are people living with dementia. They may, or may not, get your order right.
However, rest assured that even if your order is mistaken, everything on our menu is delicious and one of a kind. This, we guarantee.
“It’s OK if my order was wrong. It tastes so good anyway.” We hope this feeling of openness and understanding will spread across Japan and through the world.
At the first pop-up, 37% of the orders were mistaken. This video explains a bit more about the concept and shows the restaurant in action.
For the New Yorker, Brooke Jarvis reviews Timothy C. Winegard’s The Mosquito: A Human History of Our Deadliest Predator.
It turns out that, if you’re looking for them, the words “mosquitoes,” “fever,” “ague,” and “death” are repeated to the point of nausea throughout human history. (And before: Winegard suggests that, when the asteroid hit, dinosaurs were already in decline from mosquito-borne diseases.) Malaria laid waste to prehistoric Africa to such a degree that people evolved sickle-shaped red blood cells to survive it. The disease killed the ancient Greeks and Romans — as well as the peoples who tried to conquer them — by the hundreds of thousands, playing a major role in the outcomes of their wars. Hippocrates associated malaria’s late-summer surge with the Dog Star, calling the sickly time the “dog days of summer.” In 94 B.C., the Chinese historian Sima Qian wrote, “In the area south of the Yangtze the land is low and the climate humid; adult males die young.” In the third century, malaria epidemics helped drive people to a small, much persecuted faith that emphasized healing and care of the sick, propelling Christianity into a world-altering religion.
And then there’s this:
In total, Winegard estimates that mosquitoes have killed more people than any other single cause — fifty-two billion of us, nearly half of all humans who have ever lived. He calls them “our apex predator,” “the destroyer of worlds,” and “the ultimate agent of historical change.”
Two other recent reviews of the book: In ‘The Mosquito,’ Humans Face A Predator More Deadly Than The Rest (NPR) and The mosquito isn’t just annoying — Timothy C. Winegard says we’re at war (LA Times).
From Outside magazine, an article on what your body goes through and what it feels like to die from heat stroke. A perhaps unnecessary note: this gets intense and a little graphic.
There are two kinds of heatstroke: classic and exertional. Classic heatstroke hits the very young, the elderly, the overweight, and people suffering from chronic conditions like uncontrolled diabetes, hypertension, and cardiovascular disease. Alcohol and certain medications (diuretics, tricyclic antidepressants, antipsychotics, and some cold and allergy remedies) can increase susceptibility as well. Classic heatstroke can strike in the quiet of upper-floor apartments with no air-conditioning.
Exertional heatstroke, on the other hand, pounces on the young and fit. Exercise drastically accelerates temperature rise. Marathon runners, cyclists, and other athletes sometimes push into what used to be known as the fever of exercise and is now called exercise-induced hyperthermia, where internal temperatures typically hit 100 to 104 degrees. Usually, there’s no lasting damage. But as body temperature climbs higher, the physiological response becomes more dramatic and the complications more profound. The higher temperature can ultimately trigger a cascading disaster of events as the metabolism, like a runaway nuclear reactor, races so fast and so hot that the body can’t cool itself down. A person careens toward organ failure, brain damage, and death.
It’s a sequel of sorts to this piece about what it feels like to freeze to death, which I vividly remember reading many years ago.
At 85 degrees, those freezing to death, in a strange, anguished paroxysm, often rip off their clothes. This phenomenon, known as paradoxical undressing, is common enough that urban hypothermia victims are sometimes initially diagnosed as victims of sexual assault. Though researchers are uncertain of the cause, the most logical explanation is that shortly before loss of consciousness, the constricted blood vessels near the body’s surface suddenly dilate and produce a sensation of extreme heat against the skin.
Olga Khazan on The Reason Anxious People Often Have Allergies:
“There is good circumstantial evidence that’s growing that a number of mental illnesses are associated with immune dysfunction,” says Sandro Galea, a physician and epidemiologist at the Boston University School of Public Health.
If the link is in fact real, allergies could be causing anxiety and other mood disorders in a few different ways. For one, it’s stressful to be sick, and people with allergies frequently feel like they have a bad cold. The experience of straining to breathe, or of coughing and wheezing, could simply make people feel anxious.
Then there are biological explanations. Allergies trigger the release of the stress hormone cortisol, which can interfere with a feel-good brain chemical called serotonin. It’s not clear how the cortisol does this, Nanda says; it might inhibit the production of serotonin or make it fail to bind with its receptors properly. But when something goes wrong with serotonin, the theory goes, depression or anxiety might set in.
Huh. I definitely suffer from seasonal allergies (they have thankfully slacked off for the summer) and have struggled with anxiety since I was a kid (though I’ve never been clinically diagnosed). I’ll be following this research with interest.
According this video by Kurzgesagt (and their extensive list of sources), the answer to that question for now is: no, our electronic devices are not causing long- or short-term health problems in the brains or bodies of people who use them.
Electrosmog is one of those things that is a bit vague and hard to grasp. When personal health is involved, feelings clash extra hard with scientific facts and there is a lot of misinformation and exaggeration out there. On the other hand, some people are really worried and distressed by the electricity that surrounds them. And just to wave this off is not kind or helpful.
While there is still a lot of researching being done on the dangers of constant weak electromagnetic radiation, it is important to stress that so far, we have no reason to believe that our devices harm us. Other than… well… spending too much time with them.
Biology is one field I don’t know supremely well, having had a couple of college courses and then mostly just public television documentaries. So it’s always cool to get a new concept or two to play with, like the Hayflick Limit.
What is it?
In normal, replicating cells, all the important genetic code in a cell’s nucleus is protected by telomeres—sections of non-coding DNA on the ends of chromosomes. (Elizabeth Blackburn, who won a Nobel for her work on telomeres, compares them to the caps on the end of shoelaces that keep them from fraying.) Every time cells divide, telomeres shorten ever so slightly; the white blood cells in newborn humans have telomeres that consist of about 8,000 base pairs, which falls to around 1,500 in the elderly.
The Hayflick limit is thought to occur when telomeres are gone and cell division would be risky, because without their protection, loss of genetic information would occur. When cells no longer replicate, they’re considered “senescent”: they carry on most of their normal cellular activity and eventually die. The Hayflick limit is one cause, but external stress, like an infection, physical trauma, or UV radiation can hasten cell death, according to Jan van Deursen, a cancer biologist at the Mayo Clinic in Rochester, Minnesota.
Senescent cells are a culprit in aging, but they also have benefits. They give off proteins that can recruit immune cells, which can promote wound healing, and they’re one of our body’s defenses against cancer. One of the reasons cancer occurs is when cells switch on a gene that allows them to rebuild their telomeres—kind of like speeding through a stop sign. That’s why the only immortal human cells are cancer cells.
So the Hayflick Limit, if it could be waived, could theoretically prevent or delay aging. But as it is, it’s a built-in cap on how many replications a body’s cells and tissues can undergo, so it guarantees our mortality.
Here’s what Hayflick himself had to say about it:
To slow, or even arrest, the aging process in humans is fraught with serious problems in the relationships of humans to each other and to all of our institutions. By allowing asocial people, tyrants, dictators, mass murderers, and people who cause wars to have their longevity increased should be undesirable. Yet, that would be one outcome of being able to tamper with the aging process.
I guess at a minimum, as bad as everyone is, at least they (as an individual) are not around to be bad forever? I’ll take that silver lining.
About two weeks ago, I had my right shoulder replaced. This was the second time I’ve had surgery on that shoulder, after multiple knee surgeries and arm surgeries, and abscesses and god knows what else. This surgery took place in the middle of what’s now, to me, a very familiar, and very tedious dance with my doctors around pain, pain management, and painkillers.
The way it works is this. Everyone knows that surgery, and the injuries that lead to surgery, are painful. Everyone also knows that the best way to treat pain of this kind is through the regular administration of opiates. However, because these drugs are addictive, everyone has to act as if they don’t know anything of the kind.
So instead of just prescribing the drugs, and preventing the pain, the doctors and nurses will wait until the patient asks for the pain medication. Or they’ll prescribe pain pills, but not enough to get the patient through to the next meeting with the doctor. They put the onus on the patient to beg for relief of his/her pain. Ideally with a buffer in between, like a nurse or a pain management specialist, so that the decision never comes directly from the person you’re interacting with, but an intercessor. This is why some patients end up medicated up to the gills, and others are left to grind their teeth and just get through it.
It’s really stupid. I suspect it heightens rather than lessening patients’ feelings of dependence on these drugs, which can do so much to reduce their acute pain and chronic discomfort. Instead, they’re doled out in a semi-arbitrary fashion, generally carefully rationed but sometimes overprescribed, based on your willingness to perform pain for someone else and that person’s level of compassion or complicity with your suffering.
This is all to say: no, I’m not on pain medication. Yes, I’m terribly uncomfortable. No, I’m not uncomfortable enough to jump through hoops and beg for more drugs. (Maybe if I were, things would be different.) And at the times I was most uncomfortable, those were the times when medicine was the least available to me, by design.
We’ve got to get over our weird Puritanical crap about pain and pain medication, and accept the fact that in certain contexts, we need the drugs. And by “we,” I mean myself, the medical system; everybody. We can’t be responsible for the entire opioid epidemic every second of every day. Sometimes we just need to be able to go to sleep.
Diane Munday, an 86-year-old women’s rights activist, recalls what illegal abortion had been like in the UK in the 1960s.
“Women would drink bleach to try to induce miscarriage. They would have very hot baths, or move heavy furniture, or try to do it themselves with a needle or a crochet hook,” says Munday.
As a result, an underground network of backstreet abortionists ran quietly across the country. Some of them, says Munday, became involved by force. It was not unknown for women who had carried out abortions for their close friends and family to be blackmailed by desperate pregnant women who threatened to report them to the police if they didn’t help them, too. Like women who had abortions, those who carried out the procedure illegally could be sent to prison.
“These people were unskilled. Some might have had a bit of nursing experience or had worked in a hospital, or carried out procedures for a friend or daughter,” says Munday.
Munday became active in the campaign to legalize abortion in the UK after she had one herself following giving birth to three children in less than four years.
See also Harrowing Illegal Abortion Stories from Before Roe v. Wade.
Newer posts
Older posts
Socials & More