kottke.org posts about cancer
In a letter to the Times of London, Dr. Michael Baum tells how a line in Arcadia by Tom Stoppard sparked an idea which resulted in adjuvant systemic chemotherapy, a therapy Baum helped pioneer which greatly increased the survivability of breast cancer.
Sir, In 1993 my wife and I went to see the first production of Arcadia by Tom Stoppard (obituary, Dec 1), and in the interval I experienced a Damascene conversion. As a clinical scientist I was trying to understand the enigma of the behaviour of breast cancer, the assumption being that it grew in a linear trajectory spitting off metastases on its way. In the first act of Arcadia, Thomasina asks her tutor, Septimus: “If there is an equation for a curve like a bell, there must be an equation for one like a bluebell, and if a bluebell, why not a rose?” With that Stoppard explains chaos theory, which better explains the behaviour of breast cancer. At the point of diagnosis, the cancer must have already scattered cancer cells into the circulation that nest latent in distant organs. The consequence of that hypothesis was the birth of “adjuvant systemic chemotherapy”, and rapidly we saw a striking fall of the curve that illustrated patients’ survival.
Stoppard never learnt how many lives he saved by writing Arcadia.
Michael Baum
Professor emeritus of surgery; visiting professor of medical humanities, UCL
Certainly drives home the value of a robust and diverse culture of humanities in contradiction to the current backlash. (via @harrywallop.co.uk)
In 2010, Randall Munroe’s fiancée (now wife) was diagnosed with cancer. Every once in awhile, he updates his audience at XKCD on how that’s going. The most recent missive: Fifteen Years.

If you’re not up on XKCD lore, here’s an explanation. 💞
It’s not often that a movie trailer makes you cry — but this one might.1
Come See Me in the Good Light is a documentary film about poets Andrea Gibson and Megan Falley facing a cancer diagnosis that took Gibson’s life earlier this year.
This is the beginning of a nightmare, I thought. But stay with me, y’all, because my story is one about happiness, being easier to find, once we realize we do not have forever to find it.
Falley’s letter published just after Gibson’s death will give you a sense of the spirit of the film & the two humans at the center of it:
A couple years ago, Andrea said, “Whenever I leave this world, whether it’s sixty years from now, I wouldn’t want anyone to say I lost some battle. I’ll be a winner that day.”
Whatever beast of emotion bucks or whimpers through you right now, I hope you can hold that line beside it: Andrea didn’t lose anything. If you had been here in our home during the three days of their dying — if you’d seen dozens of friends drift in to help, to say goodbye, to say thank you, to kiss their perfect face, if you’d felt the love that floored every hospice nurse — you would have agreed. Andrea won.
The film is set to premiere Nov 14 on Apple TV.
I’d missed that Time magazine is naming a “Kid of the Year” now and this year’s recipient is 15-year-old scientist Heman Bekele, who has developed a soap that could treat and even prevent skin cancer.
A few years ago, he read about imiquimod, a drug that, among other uses, is approved to fight one form of skin cancer and has shown promise against several more. Typically, imiquimod, which can help destroy tumors and usually comes in the form of a cream, is prescribed as a front-line drug as part of a broader cancer treatment plan, but Heman wondered if it could be made available more easily to people in the earliest stages of the disease. A bar of soap, he reckoned, might be just the delivery system for such a lifesaving drug, not just because it was simple, but because it would be a lot more affordable than the $40,000 it typically costs for skin-cancer treatment.
“What is one thing that is an internationally impactful idea, something that everyone can use, [regardless of] socioeconomic class?” Heman recalls thinking. “Almost everyone uses soap and water for cleaning. So soap would probably be the best option.”
Using the metaphor of a cancerous tumor as an unruly village, Kurzgesagt explains how cancer develops in the human body, how the body fights against it, and how, sometimes, the cancer develops into something unmanageable.
In a sense this tiny tumor is like a rogue town. Imagine a group of rebels in Brooklyn decided that they were no longer part of New York but started a new settlement called Tumor Town, which happens to occupy the same space. The new city wants to grow, so it orders tons of steel beams, cement and drywall. New buildings follow no logic, are badly planned, ugly and dangerously crooked. They are built right in the middle of streets, on top of playgrounds and on existing infrastructure. The old neighborhood is torn down or overbuilt to make room for new stuff. Many of the former residents are trapped in the middle of it and begin to starve. This goes on for a while until the smell of death finally attracts attention. Building inspectors and police show up.
Last week, popular YouTuber, author, and science communicator Hank Green announced that he had cancer (very treatable Hodgkin’s lymphoma). His video announcement was part of a series of back-and-forth videos he does with his brother John Green, popular YouTuber and novelist. John replied to Hank’s video with a short one of his own, noting that humor is one way that people deal with grief but also a way in which we can accompany people through tough times.
To work, the humor has to feel like love rather than judgment, like inclusion rather than stigma, and like celebration rather than dismissal. And that’s a tough balance. Sometimes well-intentioned people, including me, get it wrong. And it also depends on, like, who’s saying it and the context.
Good luck and my warmest thoughts to the Greens and their family as they navigate this difficult time. And, you know, fuck cancer.
From Kurzgesagt, this video is a good overview of the arms race going on in all human bodies between cancer cells and the defenses developed by our immune systems over the years.
Somewhere in your body, your immune system just quietly killed one of your own cells, stopping it from becoming cancer, and saving your life. It does that all the time. The vast majority of cancer cells you develop will be killed without you ever noticing. Which is an incredibly hard job because of what cancer cells are: parts of yourself that start to behave as individuals even if it hurts you.
What is cancer and how does your body kill it all the time?
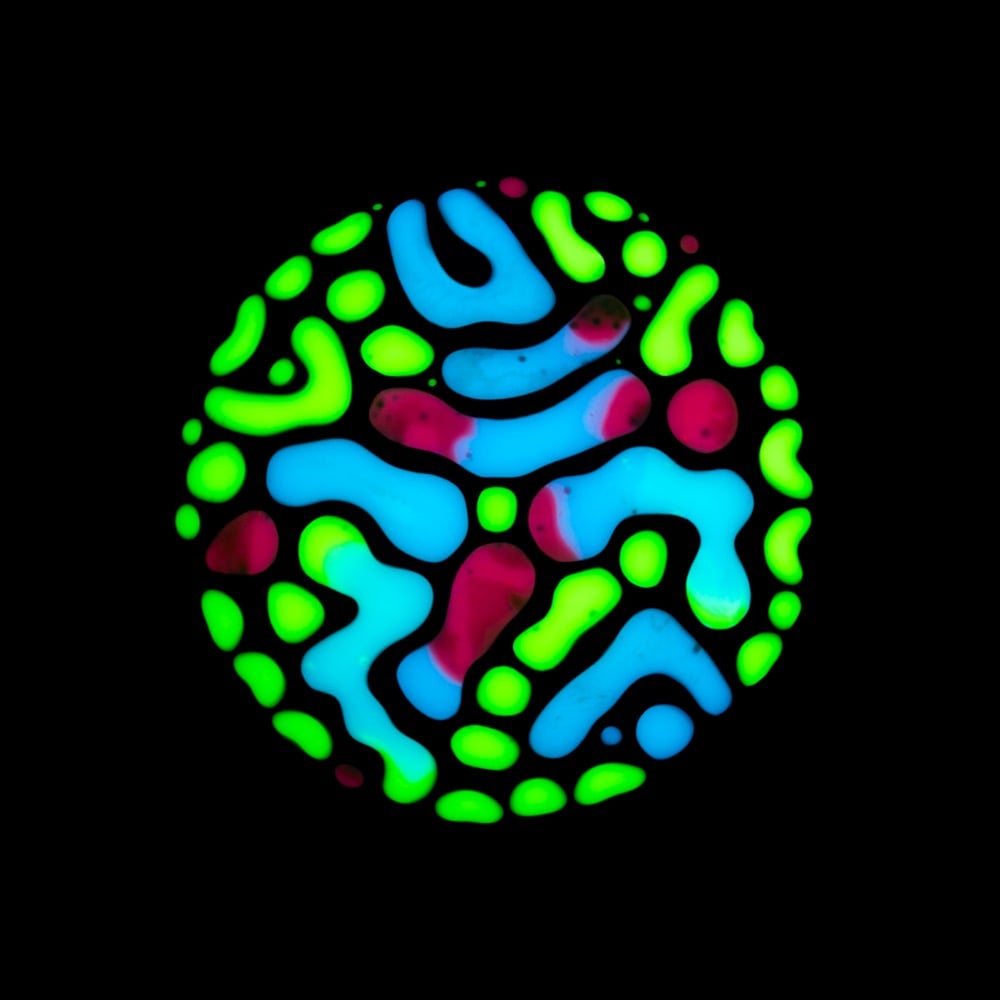
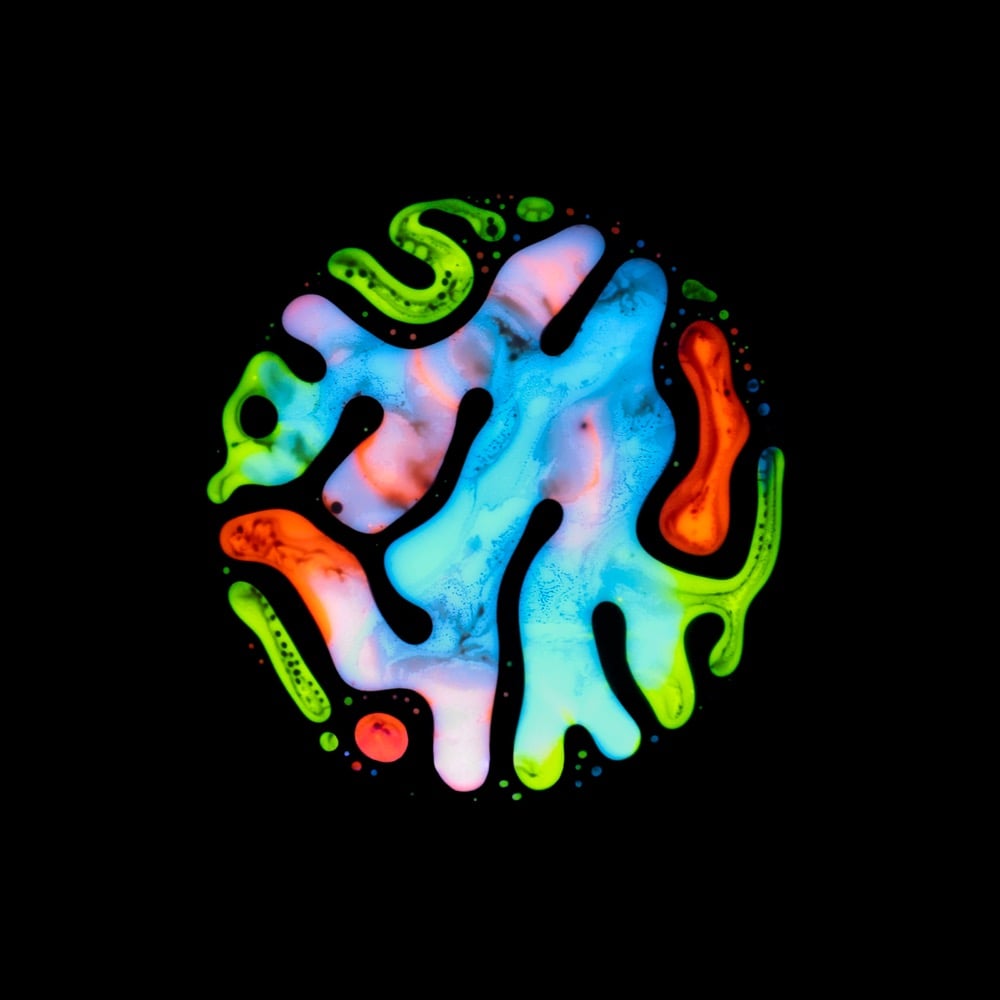
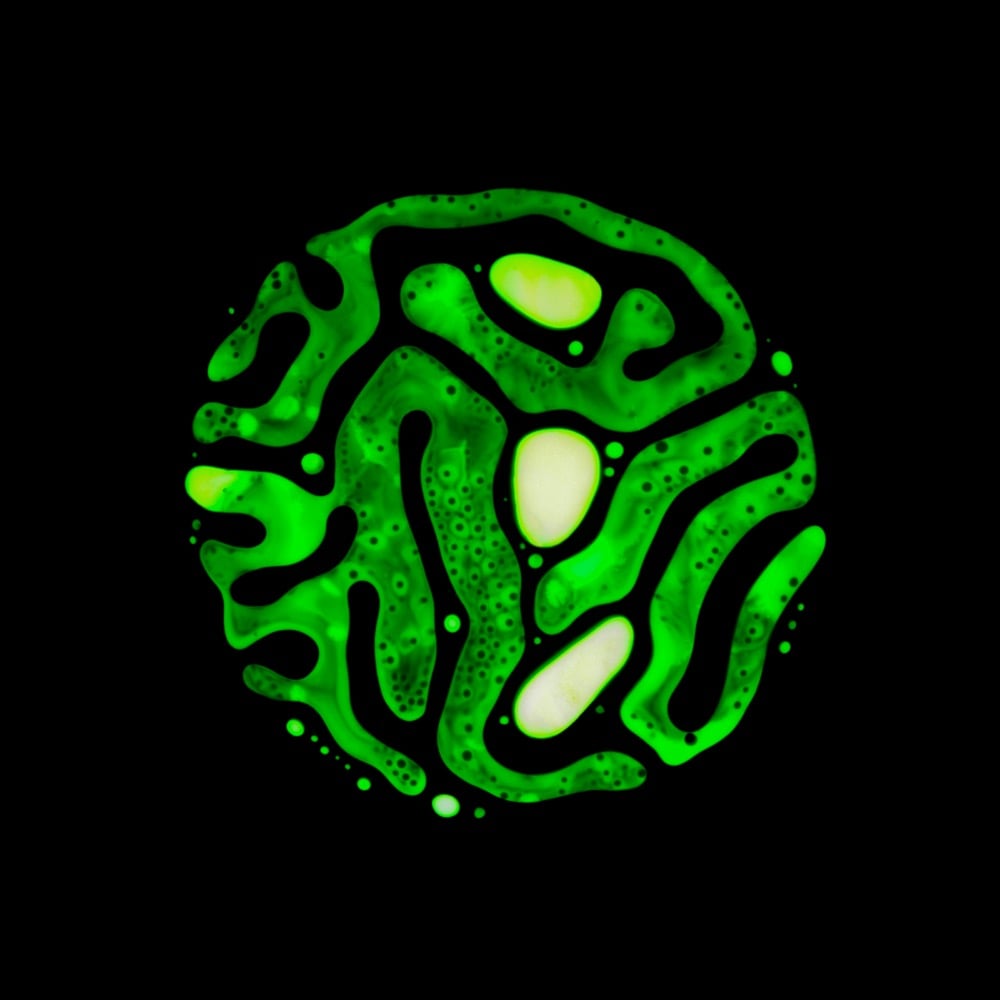

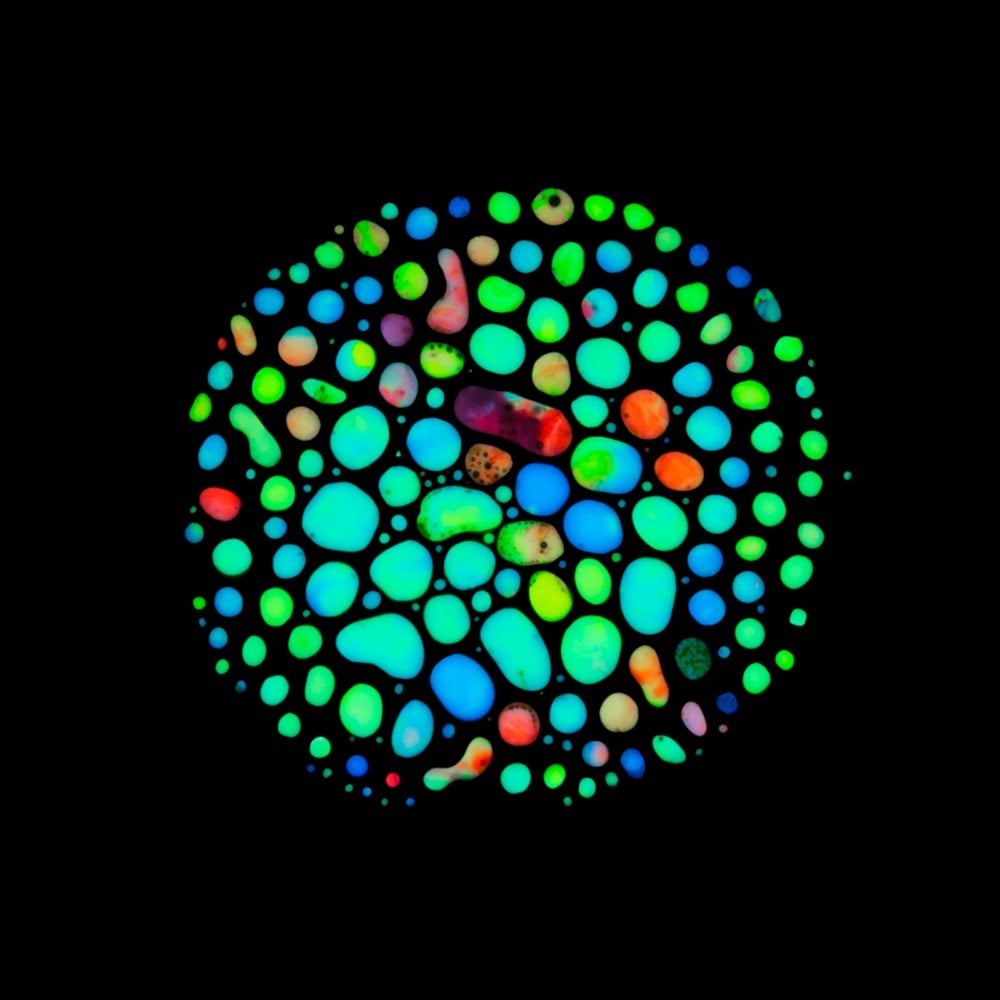
During the course of battling salivary gland tumors over many years, photographer and artist Rubén Álvarez discovered hematopoiesis (the process by which blood cells & blood plasma are formed in the body) as a possible treatment option. The treatment didn’t end up being applicable to his situation, but the process became the inspiration for a very personal project called Haematopoiesis.
This project was inspired by my very personal experiences so I discovered the Hematopoiesis process, while I was looking for treatments for more than 15 pleomorphic adenomas that were located around my head and neck. I went through several surgeries to remove them and reconstruct my facial nerve, as well as almost thirty radiotherapy sessions to prevent these adenomas to appear again.
Álvarez used paint, ferrofluid, and magnets to produce his interpretation of the actual hematopoiesis process. (via moss & fog)
In this short film by Simon Perkins, Jon Wilson shares his story of how cancer left him with one leg and the perspective he’s gained by skinning up and then skiing down mountains.
Sometimes I forget I’m broken. I cover up my scars and plug my ears. Things go okay for a while, but then I start thinking I’m entitled to some artificial slice of happiness, and before I know it I’m climbing a ladder to nowhere. To get down again, and find my equilibrium, it helps to remember when I was so low. It also helps to remind myself that life is relatively good if I have the luxury to ski up a goddamn mountain.
Many of us are scared to be broken. I’m a high school teacher, and I see it in the kids around me every day. They’re conditioned by black mirrors and social media algorithms designed for “perfect offerings.” We tell them about the ills of brokenness, but not the power and wisdom in it. We talk about post-traumatic stress — not post-traumatic growth. Being broken is a pre-existing condition that is never expunged from our record. And while I would never wish it on anyone, I would never trade in my scars, even if it meant having my leg back.

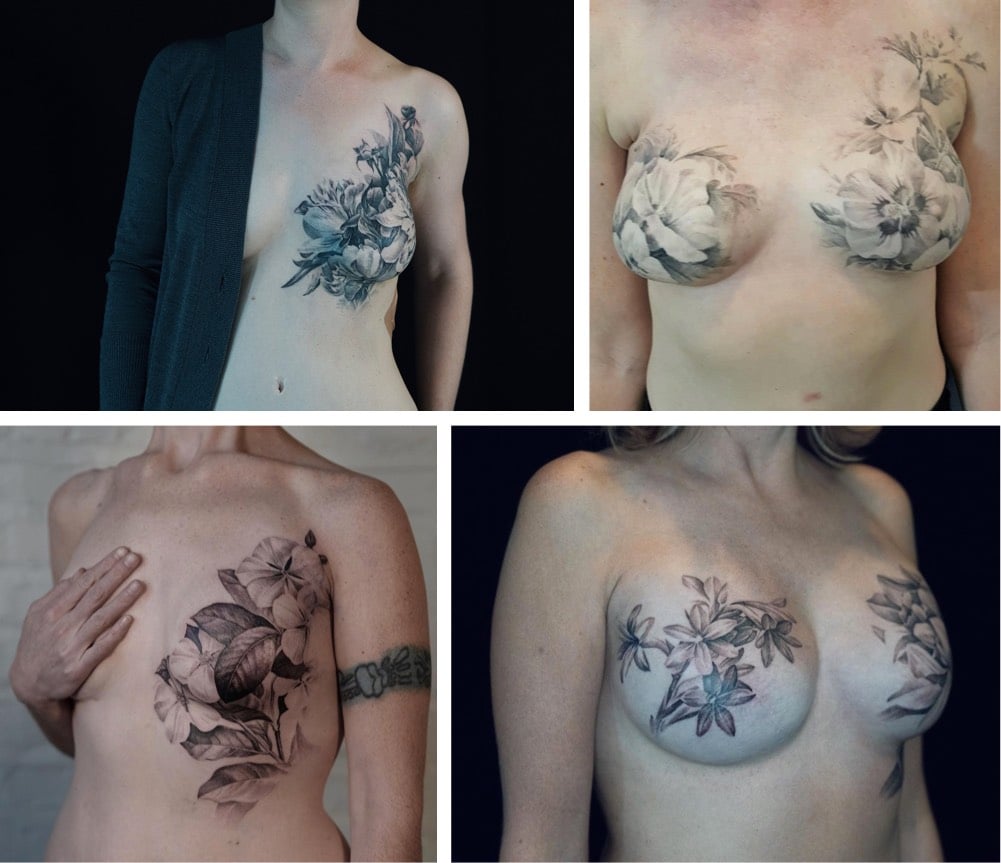
David Allen is a tattoo artist who does postmastectomy tattooing. He works with women who survive breast cancer to design and implement tattoos that cover scarring from mastectomies, transforming what might be seen as a destructive disfigurement into something creative and beautiful. Here’s Allen writing for The Journal of the American Medical Association (abstract):
I am a tattoo artist who works with women after they’ve had mastectomies to transform their sense of disfigurement and loss of control into feelings of beauty and agency. On a good day, I can heal with my art.
The women with breast cancer with whom I work share a feeling that they’ve been acted upon — by cancer, the health industrial complex and its agents, the sequelae of their treatments. Their physical and psychological points of reference are destabilized, having changed so quickly. A successful tattooing experience establishes a new point of reference, a marker that’s intimately theirs that replaces their sense of rupture and damage with an act of creation and, in my work, images of natural life.
Allen even does “solidarity tattoos” for his clients’ partners and friends. You can see more of his postmastectomy work on Instagram.
Even though larger animals like elephants and blue whales have up to 100 billion more cells than humans in their bodies — and therefore many more chances for harmful mutations to develop — they are much more immune to cancer. This is called Peto’s paradox the subject of Kurzgesagt’s latest video. Scientists aren’t sure why this happens, but one hypothesis is that in order to have grown so large, the evolutionary process that resulted in these animals provided built-in defenses against cancer that other animals didn’t need. Further reading on the topic is available here.
Biology is one field I don’t know supremely well, having had a couple of college courses and then mostly just public television documentaries. So it’s always cool to get a new concept or two to play with, like the Hayflick Limit.
What is it?
In normal, replicating cells, all the important genetic code in a cell’s nucleus is protected by telomeres—sections of non-coding DNA on the ends of chromosomes. (Elizabeth Blackburn, who won a Nobel for her work on telomeres, compares them to the caps on the end of shoelaces that keep them from fraying.) Every time cells divide, telomeres shorten ever so slightly; the white blood cells in newborn humans have telomeres that consist of about 8,000 base pairs, which falls to around 1,500 in the elderly.
The Hayflick limit is thought to occur when telomeres are gone and cell division would be risky, because without their protection, loss of genetic information would occur. When cells no longer replicate, they’re considered “senescent”: they carry on most of their normal cellular activity and eventually die. The Hayflick limit is one cause, but external stress, like an infection, physical trauma, or UV radiation can hasten cell death, according to Jan van Deursen, a cancer biologist at the Mayo Clinic in Rochester, Minnesota.
Senescent cells are a culprit in aging, but they also have benefits. They give off proteins that can recruit immune cells, which can promote wound healing, and they’re one of our body’s defenses against cancer. One of the reasons cancer occurs is when cells switch on a gene that allows them to rebuild their telomeres—kind of like speeding through a stop sign. That’s why the only immortal human cells are cancer cells.
So the Hayflick Limit, if it could be waived, could theoretically prevent or delay aging. But as it is, it’s a built-in cap on how many replications a body’s cells and tissues can undergo, so it guarantees our mortality.
Here’s what Hayflick himself had to say about it:
To slow, or even arrest, the aging process in humans is fraught with serious problems in the relationships of humans to each other and to all of our institutions. By allowing asocial people, tyrants, dictators, mass murderers, and people who cause wars to have their longevity increased should be undesirable. Yet, that would be one outcome of being able to tamper with the aging process.
I guess at a minimum, as bad as everyone is, at least they (as an individual) are not around to be bad forever? I’ll take that silver lining.
When she was 16, Charlotte Eades was diagnosed with glioblastoma, an extremely aggressive form of brain cancer. About a year after the diagnosis, she began documenting her illness and her life on her YouTube channel. After Eades died, her family made the video above, a short tribute to her life and video blog.
According to a study published in March 2017 in the Journal of the National Cancer Institute, cancer death rates continue to fall across most cancer types. From 2010 to 2014 (the most recent year that statistical data is available), overall death rates decreased by 1.8%.
Overall cancer death rates from 2010 to 2014 decreased by 1.8% (95% confidence interval [CI] = -1.8% to -1.8%) per year in men, by 1.4% (95% CI = -1.4% to -1.3%) per year in women, and by 1.6% (95% CI = -2.0% to -1.3%) per year in children. Death rates decreased for 11 of the 16 most common cancer types in men and for 13 of the 18 most common cancer types in women, including lung, colorectal, female breast, and prostate, whereas death rates increased for liver (men and women), pancreas (men), brain (men), and uterine cancers.
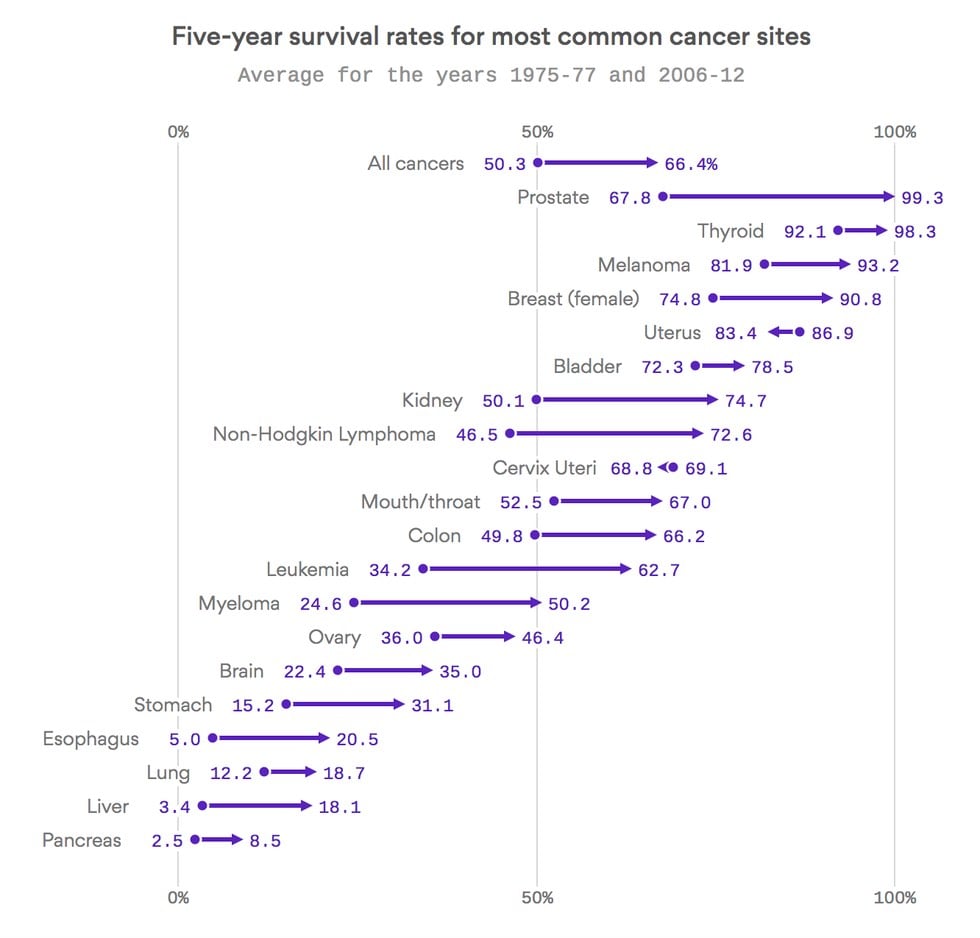
But the trends are much clearer when you look at progress over a longer time period. As this graph from Axios shows, the five-year survival rates for most common types of cancer have increased quite significantly in the past 30-40 years. Survival rates from all cancers increased by 16% and jumped 26% and almost 29% for non-Hodkin lymphoma and leukemia respectively. If you have prostate or thyroid cancer, you’re almost guaranteed to survive 5 years at this point and the female breast cancer survival rate is up to almost 91%. (via @Atul_Gawande)
Senator John McCain has been diagnosed with a particularly aggressive form of brain cancer. The tumor has been removed and McCain is recovering at home with his family. I wish Senator McCain well and hope for a speedy recovery.
In the wake of his diagnosis, many of those expressing support for McCain reference his considerable personal strength in his fight against cancer. President Obama said:
John McCain is an American hero & one of the bravest fighters I’ve ever known. Cancer doesn’t know what it’s up against. Give it hell, John.
McCain’s daughter Meghan references his toughness and fearlessness in a statement released yesterday. Vice-President Joe Biden expressed similar sentiments on Twitter:
John and I have been friends for 40 years. He’s gotten through so much difficulty with so much grace. He is strong — and he will beat this.
This is the right thing to say to those going through something like this, and hearing this encouragement and having the will & energy to meet this challenge will undoubtably increase McCain’s chances of survival. But what Biden said next is perhaps more relevant:
Incredible progress in cancer research and treatment in just the last year offers new promise and new hope. You can win this fight, John.
As with polio, smallpox, measles, and countless other diseases before it, beating cancer is not something an individual can do. Being afflicted with cancer is the individual’s burden to bear but society’s responsibility to cure. In his excellent biography of cancer from 2011, The Emperor of All Maladies, Siddhartha Mukherjee talks about the progress we’ve made on cancer:
Incremental advances can add up to transformative changes. In 2005, an avalanche of papers cascading through the scientific literature converged on a remarkably consistent message — the national physiognomy of cancer had subtly but fundamentally changed. The mortality for nearly every major form of cancer — lung, breast, colon, and prostate — had continuously dropped for fifteen straight years. There had been no single, drastic turn but rather a steady and powerful attrition: mortality had declined by about 1 percent every year. The rate might sound modest, but its cumulative effect was remarkable: between 1990 and 2005, the cancer-specific death rate had dropped nearly 15 percent, a decline unprecedented in the history of the disease. The empire of cancer was still indubitably vast — more than half a million American men and women died of cancer in 2005 — but it was losing power, fraying at its borders.
What precipitated this steady decline? There was no single answer but rather a multitude. For lung cancer, the driver of decline was primarily prevention — a slow attrition in smoking sparked off by the Doll-Hill and Wynder-Graham studies, fueled by the surgeon general’s report, and brought to its full boil by a combination of political activism (the FTC action on warning labels), inventive litigation (the Banzhaf and Cipollone cases), medical advocacy, and countermarketing (the antitobacco advertisements). For colon and cervical cancer, the declines were almost certainly due to the successes of secondary prevention — cancer screening. Colon cancers were detected at earlier and earlier stages in their evolution, often in the premalignant state, and treated with relatively minor surgeries. Cervical cancer screening using Papanicolaou’s smearing technique was being offered at primary-care centers throughout the nation, and as with colon cancer, premalignant lesions were excised using relatively minor surgeries. For leukemia, lymphoma, and testicular cancer, in contrast, the declining numbers reflected the successes of chemotherapeutic treatment. In childhood ALL, cure rates of 80 percent were routinely being achieved. Hodgkin’s disease was similarly curable, and so, too, were some large-cell aggressive lymphomas. Indeed, for Hodgkin’s disease, testicular cancer, and childhood leukemias, the burning question was not how much chemotherapy was curative, but how little: trials were addressing whether milder and less toxic doses of drugs, scaled back from the original protocols, could achieve equivalent cure rates.
Perhaps most symbolically, the decline in breast cancer mortality epitomized the cumulative and collaborative nature of these victories — and the importance of attacking cancer using multiple independent prongs. Between 1990 and 2005, breast cancer mortality had dwindled an unprecedented 24 percent. Three interventions had potentially driven down the breast cancer death rate-mammography (screening to catch early breast cancer and thereby prevent invasive breast cancer), surgery, and adjuvant chemotherapy (chemotherapy after surgery to remove remnant cancer cells).
Understanding how to defeat cancer is an instance where America’s fierce insistence on individualism does us a disservice. Individuals with freedom to pursue their own goals are capable of a great deal, but some problems require massive collective coordination and effort. Beating cancer is a team sport; it can only be defeated by a diverse collection of people and institutions working hard toward the same goal. It will take government-funded research, privately funded research, a strong educational system, philanthropy, and government agencies from around the world working together. This effort also requires a system of healthcare that’s available to everybody, not just to those who can afford it. Although cancer is not a contagious disease like measles or smallpox, the diagnosis and treatment of each and every case brings us closer to understanding how to defeat it. We make this effort together, we spend this time, energy, and money, so that 10, 20, or 30 years from now, our children and grandchildren won’t have to suffer like our friends and family do now.
Neoantigen vaccines use the DNA from a cancer patient’s own tumor to, hopefully, eradicate the cancer.
For some 50 years, cancer biologists have tried to incite the immune system to attack cancer by targeting molecules that commonly stud the surfaces of malignant cells. These “antigens” act as homing beacons that immune cells find and lock onto (much as antigens on viruses attract the immune system, the basis for preventive vaccines such as that for measles).
Trouble is, normal cells sometimes sport the same antigens as tumors, and the immune system is programmed not to attack antigens found on healthy cells. As a result, revving up the immune system to target common tumor antigens hasn’t worked, leading to a number of failed experimental cancer vaccines.
That led biologists to a different approach: siccing the immune system on antigens found only on cancer cells — and only on the cancer cells of a single patient. “It’s highly unlikely that any two patients have the same neoantigens,” said Dr. Catherine Wu of Boston’s Dana-Farber Cancer Institute. “That’s why we have an opportunity to make cancer vaccines truly personalized, loaded with patient-specific neoantigens.”

(Reminder: This is Susannah Breslin guest-blogging.)
I’m a freelance writer, but I didn’t do a lot of freelance writing this year, mostly because I’ve been working on a book. Recently, I’ve been reading various best-writing-of-the-year listicles floating around, and I wondered to myself, of the things I’d published this year, which I thought was the best of it. I thought of a piece I wrote for The Billfold back in May: “Blood Sacrifice.” It’s about having a very expensive dinner and having had cancer, and what the two have in common.
Check it out, if you’re interested.
Then a month ago, I got a note from a friend, who had a ticket to Next, and what he wanted to know was: Did I want to go? As far as restaurants go, Next is kind of a unicorn. It’s co-owned by Grant Achatz, who is a pioneer in the strange world of molecular gastronomy and the owner of Alinea, which is considered to be one of the best restaurants in the world, and Nick Kokonas, and it is so exclusive that you have to buy a ticket in advance to get into it. The date of the reservation was one week after my birthday. I fantasized that if I went, on the night that I was there, by some strange coincidence, Achatz would be there. Achatz, I knew, had had cancer, too, and, in my daydream, Achatz would come by the table, and I would motion to him, and he would bend down low, and I would tell him, in a murmuring voice, that I had had cancer, and I knew that he had had cancer, too. He would smile knowingly at me, and I would smile knowingly at him, and then he would disappear into the kitchen, and he would emerge with a plate of something that looked like a tumor splattered across porcelain, and I would eat it, and whatever it was made of (rhubarb? venison? something else entirely?), it would be delicious, and I would have eaten the tumor that had tried to eat me, metaphorically, of course, and the cycle of life would close upon itself, completing itself, like Ouroboros with his tail in his mouth rolling down a street like a wheel.
Also, this is a nice homage to The Billfold and its “certain sense of humanity.”
(Photo credit: Radio-Canada/Claude Brunet)
I don’t quite know what I’m doing to myself these days. Last night was an episode of The Americans in which a marriage was ending, another family was trying to keep itself intact, and a young boy struggles to move on after his entire family dies. This morning, I watched an episode of Mad Men in which a mother tries to reconcile her differences with her daughter in the face of impending separation. And then, the absolute cake topper, a story by Matthew Teague that absolutely wrecked me. It’s about his cancer-stricken wife and the friend who comes and rescues an entire family, which is perhaps the truest and most direct thing I’ve ever read about cancer and death and love and friendship.
Since we had met, when she was still a teenager, I had loved her with my whole self. Only now can I look back on the fullness of our affection; at the time I could see nothing but one wound at a time, a hole the size of a dime, into which I needed to pack a fistful of material. Love wasn’t something I felt anymore. It was just something I did. When I finished, I would lie next to her and use sterile cotton balls to soak up her tears. When she finally slept, I would slip out of bed and go into our closet, the most isolated room in the house. Inside, I would wrap a blanket around my head, stuff it into my mouth, lie down and bury my head in a pile of dirty clothes, and scream.
There are very specific parts of all those stories that I identify with. I struggle with friendship. And with family. I worry about my children, about my relationships with them. I worry about being a good parent, about being a good parenting partner with their mom. How much of me do I really want to impart to them? I want them to be better than me, but I can’t tell them or show them how to do that because I’m me. I took my best shot at being better and me is all I came up with. What if I’m just giving them the bad parts, without even realizing it? God, this is way too much for a Monday.
Oh, this sounds fantastic: PBS is set to air a six-hour documentary series, Cancer: The Emperor of All Maladies, starting at the end of March. How have I not heard about this before today?
This “biography” of cancer covers its first documented appearances thousands of years ago through the epic battles in the 20th century to cure, control and conquer it, to a radical new understanding of its essence. The series also features the current status of cancer knowledge and treatment — the dawn of an era in which cancer may become a chronic or curable illness rather than its historic death sentence in some forms.
The series is based on Siddhartha Mukherjee’s The Emperor of All Maladies: A Biography of Cancer, which is one of the most interesting books I’ve read in the past few years. Ken Burns is executive producing and Barak Goodman is directing.
Thanks to Sarah Klein at Redglass Pictures for letting me know about this. Redglass created a pair of videos for the series featuring Terrence Howard and Ken Jeong talking about their experiences with cancer.
Update: All three parts of the series are available on the PBS site for the next two weeks or so.
Two years ago, Angelina Jolie wrote in the NY Times1 about her choice to have a preventive double mastectomy. Today, she is back with an update on her choice to have another elective preventive surgery, the removal of her ovaries and fallopian tubes.
Two weeks ago I got a call from my doctor with blood-test results. “Your CA-125 is normal,” he said. I breathed a sigh of relief. That test measures the amount of the protein CA-125 in the blood, and is used to monitor ovarian cancer. I have it every year because of my family history.
But that wasn’t all. He went on. “There are a number of inflammatory markers that are elevated, and taken together they could be a sign of early cancer.” I took a pause. “CA-125 has a 50 to 75 percent chance of missing ovarian cancer at early stages,” he said. He wanted me to see the surgeon immediately to check my ovaries.
I went through what I imagine thousands of other women have felt. I told myself to stay calm, to be strong, and that I had no reason to think I wouldn’t live to see my children grow up and to meet my grandchildren.
I called my husband in France, who was on a plane within hours. The beautiful thing about such moments in life is that there is so much clarity. You know what you live for and what matters. It is polarizing, and it is peaceful.
A week ago, Paul Kalanithi, who was 37, died from lung cancer. He had recently finished his neurosurgery residency at Stanford and was a father to an infant daughter.
He was also a writer. If you haven’t read his “How Long Have I Got Left?” or “Before I Go,” you should.
In this video, he talks about how time changes as you face your mortality. “Clocks are now kind of irrelevant to me,” he says. “Time, where it used to have kind of a linear progression feel to it, now feels more like a space.”
Cord Jefferson with a beautiful piece about his mother, illness, and the importance and difficulty of being kind.
I’d just returned home from a meeting when she called again. It had been only a few hours since we’d last talked and, as she stammered when I picked up, my heart sank with the anticipation of more bad news. “I didn’t tell you everything I wanted to earlier,” she said after gathering her tongue. “I wanted to say that I’m scared. I know you can’t do anything to change this, but it makes me feel better to let you know that I’m afraid.”
(via @jessicalustig)
In his mid-20s, James Golding was diagnosed with cancer. In the hospital, he weighed 84 pounds and was given a 5% chance of living. Five years later, he embarked on a journey to France to break the record for most distance ridden on a bike in 7 days. This video follows Golding through his record-breaking attempt.
The video was produced by the same team that did the lovely Experiments in Speed video.
In a clinical trial at the Mayo Clinic, a woman with a type of blood cancer called myeloma was given an injection of measles virus large enough to innoculate 10 million people and has been “completely cleared” of her cancer.
So, as part of a two-patient clinical trial, doctors at the Mayo Clinic injected Erholtz with 100 billion units of the measles virus — enough to inoculate 10 million people.
Her doctor said they were entering the unknown.
Five minutes into the hour-long process, Erholtz got a terrible headache. Two hours later, she started shaking and vomiting. Her temperature hit 105 degrees, Stephen Russell, the lead researcher on the case, told The Washington Post early Thursday morning.
“Thirty-six hours after the virus infusion was finished, she told me, ‘Evan has started shrinking,’” Russell said. Over the next several weeks, the tumor on her forehead disappeared completely and, over time, the other tumors in her body did, too.
The cancer of the other person in the trial was unaffected and larger randomized trials still have to be performed, but this is encouraging news. Between this and the remission of cancer using HIV, it looks like viral therapy has a real shot at being a powerful weapon in fighting cancer.
Peter Bach, a cancer doctor, writes about losing his wife to cancer.
The streetlights in Buenos Aires are considerably dimmer than they are in New York, one of the many things I learned during my family’s six-month stay in Argentina. The front windshield of the rental car, aged and covered in the city’s grime, further obscured what little light came through. When we stopped at the first red light after leaving the hospital, I broke two of my most important marital promises. I started acting like my wife’s doctor, and I lied to her.
I had just taken the PET scan, the diagnostic X-ray test, out of its manila envelope. Raising the films up even to the low light overhead was enough for me to see what was happening inside her body. But when we drove on, I said, “I can’t tell; I can’t get my orientation. We have to wait to hear from your oncologist back home.” I’m a lung doctor, not an expert in these films, I feigned. But I had seen in an instant that the cancer had spread.
The last sentence here really got to me:
Our life together was gone, and carrying on without her was exactly that, without her. I was reminded of our friend Liz’s insight after she lost her husband to melanoma. She told me she had plenty of people to do things with, but nobody to do nothing with.
Bach’s discussion of treatment options reminded me of Siddhartha Mukherjee’s The Emperor of All Maladies, which is one of my favorite books of recent years. I was also reminded of how doctors die.
In a unanimous decision, the US Supreme Court ruled today that human genes cannot be patented.
The case involved Myriad Genetics Inc., which holds patents related to two genes, known as BRCA1 and BRCA2, that can indicate whether a woman has a heightened risk of developing breast cancer or ovarian cancer.
Justice Clarence Thomas, writing for the court, said the genes Myriad isolated are products of nature, which aren’t eligible for patents.
The high court’s ruling was a win for a coalition of cancer patients, medical groups and geneticists who filed a lawsuit in 2009 challenging Myriad’s patents. Thanks to those patents, the Salt Lake City company has been the exclusive U.S. commercial provider of genetic tests for breast cancer and ovarian cancer.
The challengers argued the patents have allowed Myriad to dictate the type and terms of genetic screening available for the diseases, while also dissuading research by other laboratories.
Fuck yes. A defect in her BRCA1 gene is what caused Angelina Jolie to recently have a preventive double mastectomy. (via @tylercowen)
In this morning’s NY Times, Angelina Jolie writes about her decision to have a preventive double mastectomy to hopefully ward off cancer.
My mother fought cancer for almost a decade and died at 56. She held out long enough to meet the first of her grandchildren and to hold them in her arms. But my other children will never have the chance to know her and experience how loving and gracious she was.
We often speak of “Mommy’s mommy,” and I find myself trying to explain the illness that took her away from us. They have asked if the same could happen to me. I have always told them not to worry, but the truth is I carry a “faulty” gene, BRCA1, which sharply increases my risk of developing breast cancer and ovarian cancer.
It happens that just last night I read about the BRCA-1 gene in Siddhartha Mukhergee’s excellent biography of cancer, The Emperor of All Maladies. This part is right near the end of the book:
Like cancer prevention, cancer screening will also be reinvigorated by the molecular understanding of cancer. Indeed, it has already been. The discovery of the BRCA genes for breast cancer epitomizes the integration of cancer screening and cancer genetics. In the mid-1990s, building on the prior decade’s advances, researchers isolated two related genes, BRCA-1 and BRCA-2, that vastly increase the risk of developing breast cancer. A woman with an inherited mutation in BRCA-1 has a 50 to 80 percent chance of developing breast cancer in her lifetime (the gene also increases the risk for ovarian cancer), about three to five times the normal risk. Today, testing for this gene mutation has been integrated into prevention efforts. Women found positive for a mutation in the two genes are screened more intensively using more sensitive imaging techniques such as breast MRI. Women with BRCA mutations might choose to take the drug tamoxifen to prevent breast cancer, a strategy shown effective in clinical trials. Or, perhaps most radically, women with BRCA mutations might choose a prophylactic mastectomy of both breasts and ovaries before cancer develops, another strategy that dramatically decreases the chances of developing breast cancer.
Radical is an understatement…what a tough and brave decision to make. Again from the book, I liked this woman’s take on it:
An Israeli woman with a BRCA-1 mutation who chose this strategy after developing cancer in one breast told me that at least part of her choice was symbolic. “I am rejecting cancer from my body,” she said. “My breasts had become no more to me than a site for my cancer. They were of no more use to me. They harmed my body, my survival. I went to the surgeon and asked him to remove them.”
The genetic testing company 23andme screens for three common types of mutation in the BRCA1 or BRCA2 genes:
Five to 10 percent of breast cancers occur in women with a genetic predisposition for the disease, usually due to mutations in either the BRCA1 or BRCA2 genes. These mutations greatly increase not only the risk for breast cancer in women, but also the risk for ovarian cancer in women as well as prostate and breast cancer among men. Hundreds of cancer-associated BRCA1 and BRCA2 mutations have been documented, but three specific BRCA mutations are worthy of note because they are responsible for a substantial fraction of hereditary breast cancers and ovarian cancers among women with Ashkenazi Jewish ancestry. The three mutations have also been found in individuals not known to have Ashkenazi Jewish ancestry, but such cases are rare.
23andme testing kits are only $99.
Update: Two things. First, and I hope this isn’t actually necessary because you are all intelligent people who can read things and make up your own minds, but let me just state for the official record that you should never never never never NEVER take medical advice, inferred or otherwise, from celebrities or bloggers. Come on, seriously. If you’re concerned, go see a doctor.
Two: I have no idea what the $99 23andme test covers with regard to BRCA1 and BRCA2 gene mutations beyond what the company states. The most comprehensive test for BRCA1 and BRCA2 mutations was developed by a company called Myriad Genetics and costs about $3000. Myriad has patented the genes, a decision that has been sharply criticized and is currently being decided by the Supreme Court.
But many doctors, patients and scientists aren’t happy with the situation.
Some are offended by the very notion that a private company can own a patent based on a gene that was invented not by researchers in a lab but by Mother Nature. Every single cell in every single person has copies of the BRCA1 and BRCA2 genes.
Myriad officials say they deserves the patent because they invested a great deal of money to figure out the sequence and develop “synthetic molecules” based on that sequence that can be used to test the variants in a patient.
“We think it is right for a company to be able to own its discoveries, earn back its investment, and make a reasonable profit,” the company wrote on its blog.
I do know the 23andme test covers something related to the BRCA1 and BRCA2 mutations…a friend of a friend did the 23andme test, tested positive for the BRCA1 mutation, and decided to have a preventive double mastectomy after consulting her doctor and further tests. (thx, mark, allison, and ★spavis)
Sad news from Chicago: Roger Ebert’s cancer has returned and he’s taking what he calls a “leave of presence” to focus on recovery and a few different projects.
What in the world is a leave of presence? It means I am not going away. My intent is to continue to write selected reviews but to leave the rest to a talented team of writers handpicked and greatly admired by me. What’s more, I’ll be able at last to do what I’ve always fantasized about doing: reviewing only the movies I want to review.
At the same time, I am re-launching the new and improved Rogerebert.com and taking ownership of the site under a separate entity, Ebert Digital, run by me, my beloved wife, Chaz, and our brilliant friend, Josh Golden of Table XI. Stepping away from the day-to-day grind will enable me to continue as a film critic for the Chicago Sun-Times, and roll out other projects under the Ebert brand in the coming year.
Love that first sentence. Get well soon, Roger.
I’m currently reading The Emperor of All Maladies: A Biography of Cancer (which is excellent) and I’m up to the chapters on prevention, specifically the prevention of lung cancer through reduction of cigarette smoking. I had no idea cigarette smoking was so uncommon in the US as recently as 1870…but we caught up quickly.
In 1870, the per capita consumption in America was less than one cigarette per year. A mere thirty years later, Americans were consuming 3.5 billion cigarettes and 6 billion cigars every year. By 1953, the average annual consumption of cigarettes had reached thirty-five hundred per person. On average, an adult American smoked ten cigarettes every day, an average Englishman twelve, and a Scotsman nearly twenty.
For some context on that 3500/yr per person number (and the unbelievable 7000/yr Scottish rate), the current rate in the US is around 1000/yr and the highest current rate in the world is in Serbia at almost 2900/yr per person.
Long-time crossword puzzle builder John Graham (aka Araucaria) is dying of esophageal cancer and used a crossword puzzle in the Guardian to reveal the news.
Above cryptic crossword No 25,842 sat a set of special instructions: “Araucaria,” it said, “has 18 down of the 19, which is being treated with 13 15”.
Those who solved the puzzle found the answer to 18 was cancer, to 19 oesophagus, and to 13 15 palliative care. The solutions to some of the other clues were: Macmillan, nurse, stent, endoscopy, and sunset.
Speaking from his home in Cambridgeshire, Araucaria said this particular puzzle had not taken him very long, adding that a crossword had seemed the most fitting way to make the announcement.
“It seemed the natural thing to do somehow,” he said. “It just seemed right.”
(via @daveg)
Older posts
Socials & More