kottke.org posts about healthcare
The main point of Adam Bonica’s post The Wall Looks Permanent Until It Falls is about the optimism of this moment: that the US could be ripe for a Berlin Wall-falling moment that opens the door for a better future. I’m not in the mood for that message these days (IMO, our Wall-falling is a ways off in the future), but Bonica’s analysis of how the US compares to 30 other wealthy democracies, our economic peers, is important.
Start with work and economic life. Americans work longer hours, pay more out-of-pocket for college and childcare, lack parental leave, and enjoy less economic mobility. The share of income going to the top 1 percent is nearly double the OECD average. American CEOs earn, on average, 354 times as much as their workers. More workers are trapped in poverty-wage jobs. Collective bargaining covers fewer workers. And social protections are less generous for those who fall on hard times, with the government raising less in taxes and spending more on the military.
The economy is just the beginning.
We spend nearly twice as much on healthcare as other wealthy countries do. Yet life expectancy is well below average, infant and maternal mortality rates are alarmingly high, and more Americans remain uninsured.
We suffer from overlapping public health crises — the highest rates of teenage births, drug overdoses, obesity, and gun deaths among peer nations.
His description of our unique exceptionalism goes on for several more paragraphs. But then he does something quite simple and revealing: he does the math and imagines, in concrete terms, what the US would be like if it were just an average country in its cohort. Bonica calls it “Latent America: the nation that would exist if our democracy functioned to serve the public rather than protect the already powerful”. Here’s part of his analysis:
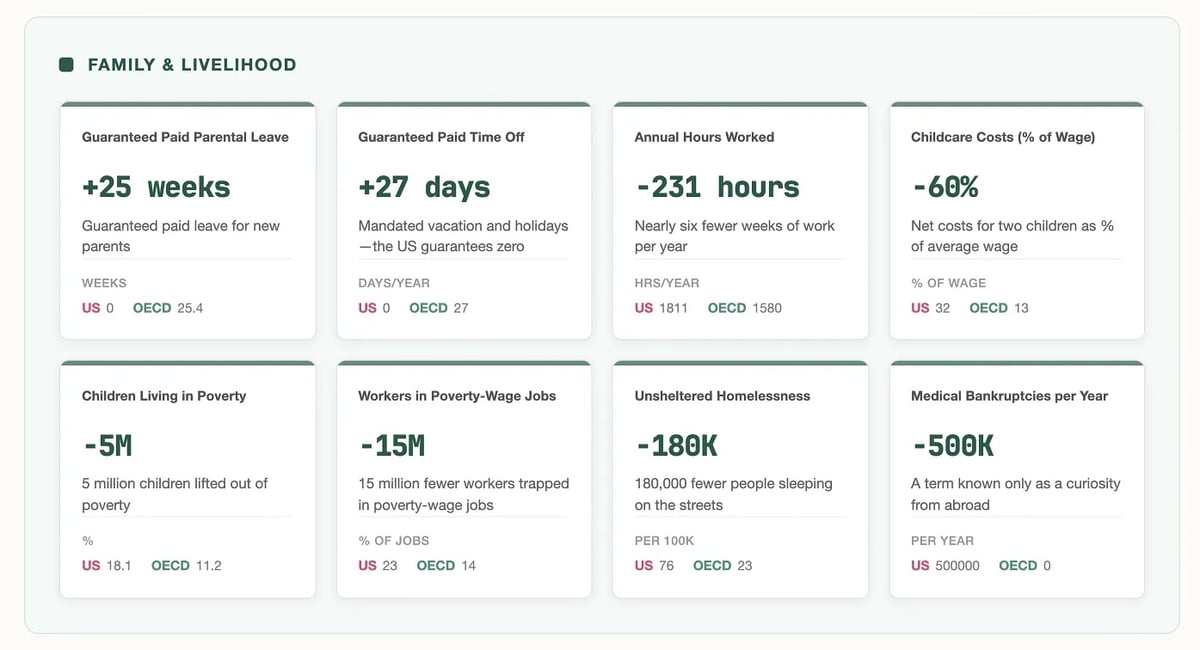
I don’t think I’ve seen this analysis done in quite this way before. You should click through to see the whole graphic, but some of the other stats are:
- $19,000 added income per household per year (and $96K more wealth)
- $2.1 trillion less spending on healthcare
- 4.1 more years of life expectancy at birth
- 51 million more Americans voting
- 1.4 million fewer Americans behind bars
- 60 more women serving in Congress
And this is just if the US were an average nation. Imagine if the US took its exceptionalism seriously and tried to maximally improve the lives of its citizens & residents instead of generating, as Bonica puts it, “enormous prosperity while deliberately withholding it from those who need it most”.
Dr. Katelyn Jetelina (aka Your Local Epidemiologist) has a frustrating update on how Covid vaccines are probably going to work this fall under the ideologically corrupt Trump regime.
The FDA is expected to license the Covid-19 vaccine. Word is that the label will be restricted to adults 65+ and people at high risk.
The Vaccine Integrity Project and professional organizations likely won’t align with RFK Jr.’s FDA license, which will cause confusion.
If you’re younger than 65 and don’t have a chronic condition, could you still get it after the label change?
Yes, but it will be complicated. While a provider could prescribe it off-label, in practice, it’s likely that most people won’t be able to access it that way.
Jetelina continues:
If you’re under 65 and not high risk, the window to get a Covid-19 vaccine is right now — before the FDA label changes. Once it happens, access will be limited immediately (if it isn’t already). CVS is no longer booking appointments. As far as we know, Walgreens and local pharmacies still are.
That was as of Monday — no idea if that’s still the case. And of course, because this is the United States, insurance will probably be a mess too:
Recommendations from these two organizations are really important for insurers. The hope is they see them and cover all vaccines, regardless of what RFK does. It also provides extra information to physicians who will prescribe off-label if RFK Jr’s FDA changes the label (as expected) this Friday.
We will not know if any of these recommendations affect insurance coverage until insurance companies confirm coverage.
[insert a lot of profanity here; seriously, this makes me so incandescently mad that if I wrote anything more it would contain every fucking swear word I know and then some]
Sources: Aug 18 thread on Bluesky, Aug 20 thread on Bluesky, Aug 18 newsletter.
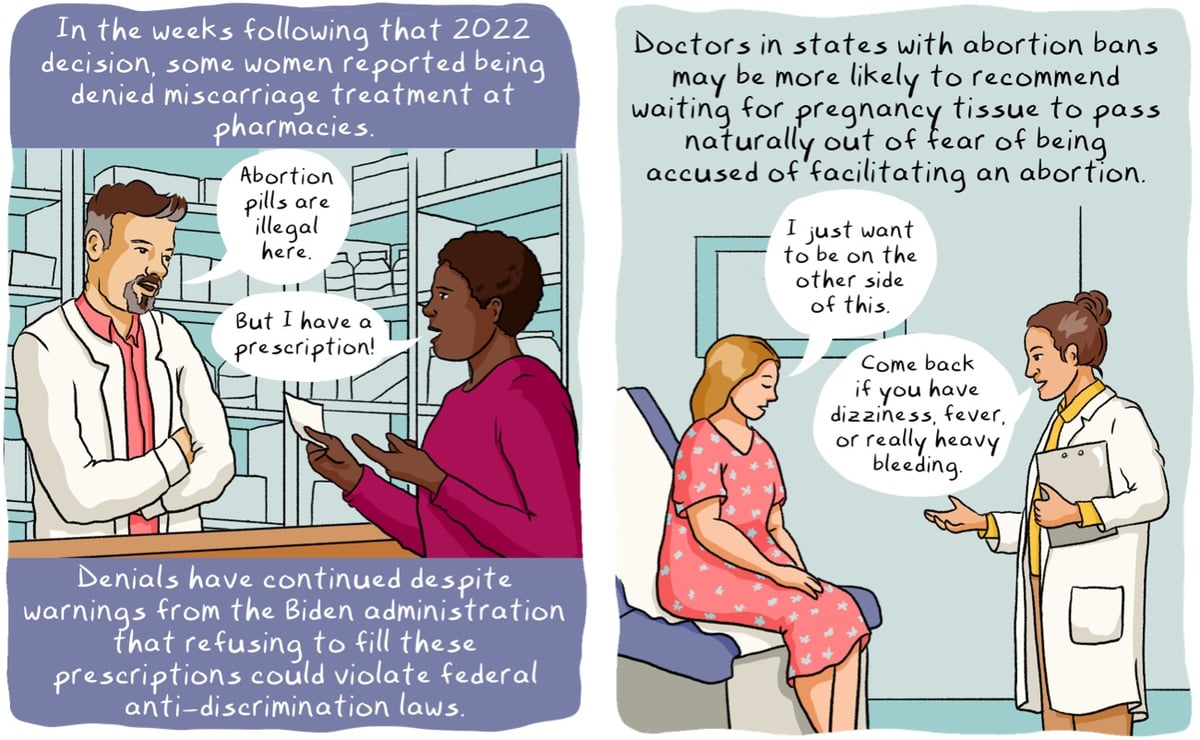
From Aubrey Hirsch, It Could Be Much, Much Worse, an illustrated guide to what health care and insurance was like in the US before the ACA.


You can also find this guide on Instagram.
In the wake of the murder of UnitedHealthcare’s CEO, a book published in 2010 by Rutgers Law professor Jay Feinman has hit the bestseller charts: Delay, Deny, Defend: Why Insurance Companies Don’t Pay Claims and What You Can Do About It. The book’s title is a reference to an insurance industry strategy of denying legitimate claims to boost profits. Bullet casings at the scene of the shooting referenced the same strategy: they were labelled “deny”, “defend”, and “depose”.
The introduction to the book is available online and it describes the origin of delay, deny, defend:
Delay, deny, defend violates the rules for handling claims that are recognized by every company, taught to adjusters, and embodied in law. Within the vast bureaucracy of insurance companies, actuaries assess risks, underwriters price policies and evaluate prospective policyholders, and agents market policies. The claims department’s only job is to pay what is owed, no more but no less. A classic text used to train adjusters, James Markham’s The Claims Environment, states the principle: “The essential function of a claim department is to fulfill the insurance company’s promise, as set forth in the insurance policy… The claim function should ensure the prompt, fair, and efficient delivery of this promise.”
Beginning in the 1990s, many major insurance companies reconsidered this understanding of the claims process. The insight was simple. An insurance company’s greatest expense is what it pays out in claims. If it pays out less in claims, it keeps more in profits. Therefore, the claims department became a profit center rather than the place that kept the company’s promise.
A major step in this shift occurred when Allstate and other companies hired the megaconsulting firm McKinsey & Company to develop new strategies for handling claims. McKinsey saw claims as a “zero-sum game,” with the policyholder and the company competing for the same dollars. No longer would each claim be treated on its merits. Instead, computer systems would be put in place to set the amounts policyholders would be offered, claimants would be deterred from hiring lawyers to help with their claims, and settlements would be offered on a take-it-or-litigate basis. If Allstate moved from “Good Hands” to “Boxing Gloves,” as McKinsey described it, policyholders would either take a lowball offer from the good hands people or face the boxing gloves of extended litigation.
I don’t know about you, but the violence implied by the “Boxing Gloves” metaphor is particularly galling — but also germane to the national conversation we’re currently having about violence, culpability, and who is and isn’t sanctioned by the state to decide who suffers or dies.

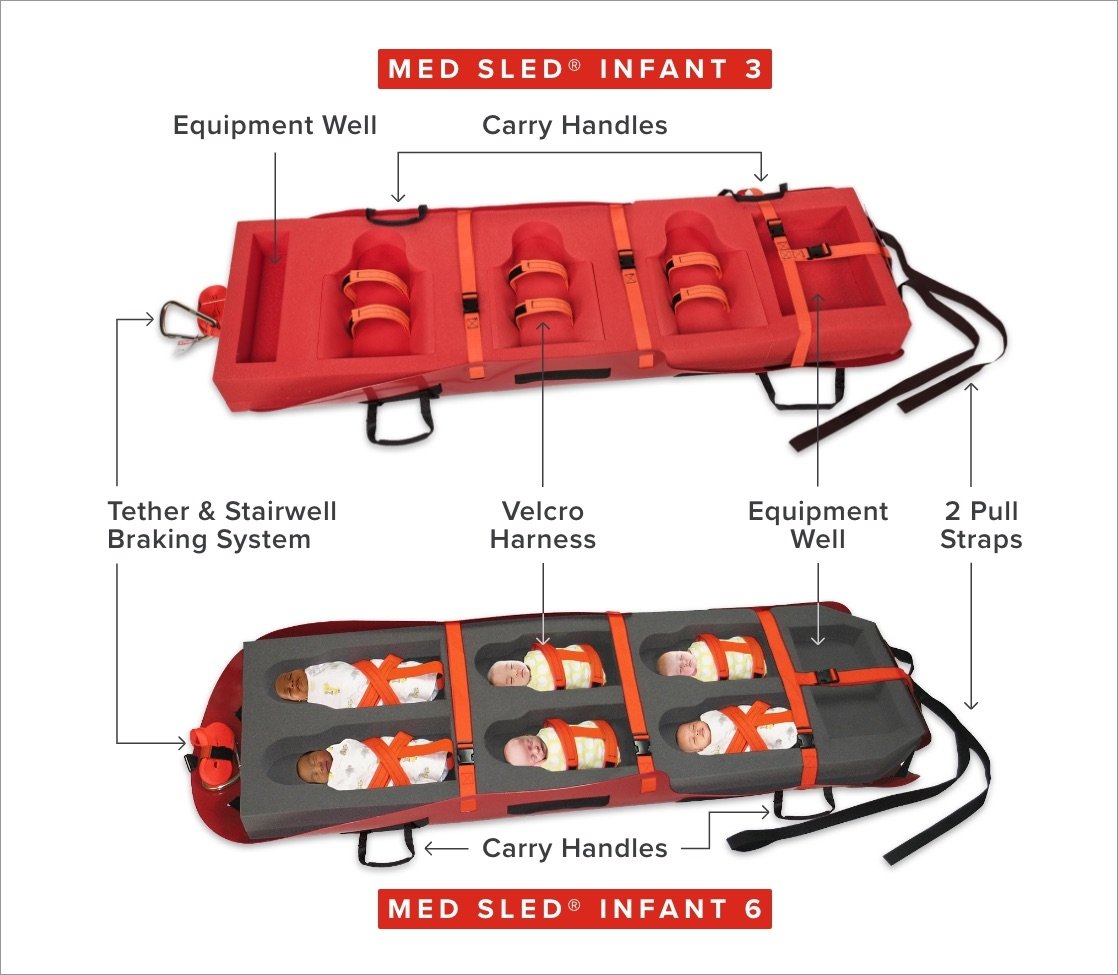
Today I learned about evacuation aprons, which places like maternity wards use to rescue infants and toddlers in case of emergency or fire. Or as this labor & delivery nurse on Threads put it:
…the goal is to grab your vest and just stuff as many babies as humanly possible in its giant kangaroo pockets before running out the door.
This particular company sells a few different models, like this apron for newborns and this one for larger infants and toddlers that can carry a total weight of 60 lbs. All the aprons are fire-resistant.
There is also something called the Med Sled, which can carry up to 6 infants at a time.
Many Patients Don’t Survive End-Stage Poverty by Dr. Lindsay Ryan is a great/upsetting piece about how the poverty many Americans are subjected to in America is killing them. Many people die here in the world’s richest country not because they are sick but because they are poor and our systems of government, justice, business, and health care don’t do enough to help them (or, more cynically and perhaps truthfully, actively work against helping them).
This is one of those pieces where I want to quote every single paragraph, but I’ll start with this one (bold mine):
Safety-net hospitals and clinics care for a population heavily skewed toward the poor, recent immigrants and people of color. The budgets of these places are forever tight. And anyone who works in them could tell you that illness in our patients isn’t just a biological phenomenon. It’s the manifestation of social inequality in people’s bodies.
I have not been able to stop thinking about this phrase since I read it: “Illness in our patients isn’t just a biological phenomenon. It’s the manifestation of social inequality in people’s bodies.”
Medical textbooks usually don’t discuss fixing your patient’s housing. They seldom include making sure your patient has enough food and some way to get to a clinic. But textbooks miss what my med students don’t: that people die for lack of these basics.
People struggle to keep wounds clean. Their medications get stolen. They sicken from poor diet, undervaccination and repeated psychological trauma. Forced to focus on short-term survival and often lacking cellphones, they miss appointments for everything from Pap smears to chemotherapy. They fall ill in myriad ways — and fall through the cracks in just as many.
You should read the whole thing yourself (NY Times gift link). Her argument about the need to expand/shift the definition of what healthcare is (e.g. housing is healthcare) reminds me of this more progressive idea of freedom.
Using a phrase popularized by reproductive justice activist Renee Bracey Sherman, The National Network of Abortion Funds teamed up with Molly Crabapple and Padma Lakshmi to produce a video about their mission to support abortion access in the US.
In order for abortion to be truly an option, it must not only be legal, but actually available, without the shame. It’s time we worked together towards a world where all people have the power and resources to care for and support their bodies, identities, and health — for themselves and their families. We need to take the hassle, hustle, and harassment out of healthcare. It’s time to change the conversation about abortion, to make it a real option, available to all people without shame or judgment. We all love someone who has had an abortion, whether we know it or not.
The video is three years old and from the very first line (“Abortion is legal in all 50 states”), you can tell how much the situation has changed in the United States — and how the NNAF’s mission is even more urgent. If you’d like to join me in donating, step right this way.
In his newest piece for The Atlantic, Ed Yong explores why, despite more than 6 million official deaths worldwide and almost a million official deaths in the US, the toll of the pandemic isn’t provoking a massive social reckoning. This is a hell of an opening paragraph:
The United States reported more deaths from COVID-19 last Friday than deaths from Hurricane Katrina, more on any two recent weekdays than deaths during the 9/11 terrorist attacks, more last month than deaths from flu in a bad season, and more in two years than deaths from HIV during the four decades of the AIDS epidemic. At least 953,000 Americans have died from COVID, and the true toll is likely even higher because many deaths went uncounted. COVID is now the third leading cause of death in the U.S., after only heart disease and cancer, which are both catchall terms for many distinct diseases. The sheer scale of the tragedy strains the moral imagination. On May 24, 2020, as the United States passed 100,000 recorded deaths, The New York Times filled its front page with the names of the dead, describing their loss as “incalculable.” Now the nation hurtles toward a milestone of 1 million. What is 10 times incalculable?
And it just keeps going from there — this is one of those articles so well written and packed with so much information and insight that it’s difficult not to quote the whole thing, even though it paints a bleak picture of America. Read the whole thing here. See also Yong’s accompanying Twitter thread.
For The Atlantic, Ed Yong writes about an idea that has gained a certain amount of traction in recent weeks as hospital systems have been overwhelmed by the Omicron surge: medical care for unvaccinated people should be limited. Yong says that’s a very bad idea:
I ran this argument past several ethicists, clinicians, and public-health practitioners. Many of them sympathized with the exasperation and fear behind the sentiment. But all of them said that it was an awful idea — unethical, impractical, and founded on a shallow understanding of why some people remain unvaccinated.
“It’s an understandable response out of frustration and anger, and it is completely contrary to the tenets of medical ethics, which have stood pretty firm since the Second World War,” Matt Wynia, a doctor and ethicist at the University of Colorado, told me. “We don’t use the medical-care system as a way of meting out justice. We don’t use it to punish people for their social choices.” The matter “is pretty cut-and-dry,” Sara Murray, a hospitalist at UC San Francisco, added. “We have an ethical obligation to provide care for people regardless of the choices they made, and that stands true for our unvaccinated patients.”
Unvaccinated people are unvaccinated for a wide variety of reasons, many of them structural constraints beyond their control. Yong connects the care of the unvaccinated to the difficulty in receiving quality care already faced by women, Black people, and disabled people:
As health-care workers become more exhausted, demoralized, and furious, they might also unconsciously put less effort into treating unvaccinated patients. After all, implicit biases mean that many groups of people already receive poorer care despite the ethical principles that medicine is meant to uphold. Complex illnesses that disproportionately affect women, such as myalgic encephalomyelitis, dysautonomia, and now long COVID, are often dismissed because of stereotypes of women as hysterical and overly emotional. Black people are undertreated for pain because of persistent racist beliefs that they are less sensitive to it or have thicker skin. Disabled people often receive worse care because of ingrained beliefs that their lives are less meaningful. These biases exist-but they should be resisted. “Stigma and discrimination as a prism for allocating health-care services is already embedded in our society,” Goldberg told me. “The last thing we should do is to celebrate it.”
That is a compelling argument and provides a necessary dose of empathy for those of us who might feel betrayed by people who are unvaccinated at this point in the pandemic. Blaming individuals for these collective responsibilities and failures is of a kind with asserting that mask-wearing and vaccination are solely personal choices rather than necessary collective actions to be undertaken by communities to keep people safer. This is the same sort of individualist thinking that has people focused on their personal “carbon footprint” instead of what massive corporations, high-emissions industries, and governments should be doing to address the climate crisis.
This is such an interesting article on vaccine avoidance in America by a primary care doctor & sociologist who have studied the phenomenon in America and other places. As more data has come in about the pandemic and vaccination program, the main differentiator in whether someone is willing to get a vaccine or not is class.
Over the past four decades, governments have slashed budgets and privatized basic services. This has two important consequences for public health. First, people are unlikely to trust institutions that do little for them. And second, public health is no longer viewed as a collective endeavor, based on the principle of social solidarity and mutual obligation. People are conditioned to believe they’re on their own and responsible only for themselves. That means an important source of vaccine hesitancy is the erosion of the idea of a common good.
Americans began thinking about health care decisions this way only recently; during the 1950s polio campaigns, for example, most people saw vaccination as a civic duty. But as the public purse shrunk in the 1980s, politicians insisted that it’s no longer the government’s job to ensure people’s well-being; instead, Americans were to be responsible only for themselves and their own bodies. Entire industries, such as self-help and health foods, have sprung up on the principle that the key to good health lies in individuals making the right choices.
Almost more than anything else, the pandemic has shown how damaged the US is from decades of neglect of the common good and how vulnerable we are to things like disease and political coups.
Ed Yong: We’re Already Barreling Toward the Next Pandemic. The US is throwing too little money at high-tech, ultimately private sector solutions but much of the problem comes down to our underfunded public health system and “profoundly unequal society”.
“To be ready for the next pandemic, we need to make sure that there’s an even footing in our societal structures,” Seema Mohapatra, a health-law expert at Indiana University, told me. That vision of preparedness is closer to what 19th-century thinkers lobbied for, and what the 20th century swept aside. It means shifting the spotlight away from pathogens themselves and onto the living and working conditions that allow pathogens to flourish. It means measuring preparedness not just in terms of syringes, sequencers, and supply chains but also in terms of paid sick leave, safe public housing, eviction moratoriums, decarceration, food assistance, and universal health care. It means accompanying mandates for social distancing and the like with financial assistance for those who might lose work, or free accommodation where exposed people can quarantine from their family. It means rebuilding the health policies that Reagan began shredding in the 1980s and that later administrations further frayed. It means restoring trust in government and community through public services. “It’s very hard to achieve effective containment when the people you’re working with don’t think you care about them,” Arrianna Marie Planey, a medical geographer at the University of North Carolina at Chapel Hill, told me.
By making public health central to their health care system, Costa Rica has achieved a higher life expectancy than the US for a fraction of the cost. How did they do it? The New Yorker’s Atul Gawande investigates.
Life expectancy tends to track national income closely. Costa Rica has emerged as an exception. Searching a newer section of the cemetery that afternoon, I found only one grave for a child. Across all age cohorts, the country’s increase in health has far outpaced its increase in wealth. Although Costa Rica’s per-capita income is a sixth that of the United States — and its per-capita health-care costs are a fraction of ours — life expectancy there is approaching eighty-one years. In the United States, life expectancy peaked at just under seventy-nine years, in 2014, and has declined since.
People who have studied Costa Rica, including colleagues of mine at the research and innovation center Ariadne Labs, have identified what seems to be a key factor in its success: the country has made public health — measures to improve the health of the population as a whole — central to the delivery of medical care. Even in countries with robust universal health care, public health is usually an add-on; the vast majority of spending goes to treat the ailments of individuals. In Costa Rica, though, public health has been a priority for decades.
The Covid-19 pandemic has revealed the impoverished state of public health even in affluent countries — and the cost of our neglect. Costa Rica shows what an alternative looks like. I travelled with Álvaro Salas to his home town because he had witnessed the results of his country’s expanding commitment to public health, and also because he had helped build the systems that delivered on that commitment. He understood what the country has achieved and how it was done.
In the US, the pandemic has revealed a public health system that is underfunded, underutilized, undervalued, and disconnected from the largely private health care system. As with many other aspects of American life, private individuals who can afford it get access to better lives, at the expense of everyone else.
The concern with the U.S. health system has never been about what it is capable of achieving at its best. It is about the large disparities we tolerate. Higher income, in particular, is associated with much longer life. In a 2016 study, the Harvard economist Raj Chetty and his research team found that the difference in life expectancy between forty-year-olds in the top one per cent of American income distribution and in the bottom one per cent is fifteen years for men and ten years for women.
So, I got a link to this video from a reader and didn’t know anything about it going in, aside from the title (“Chris Finds Out If He Has HIV”) and the reader’s comment (“American health care system”). Here’s the deal — radiologist Dr. Chris Nicholas was accidentally exposed to HIV at work and this video documents a twin journey: 1) he learns way more about HIV/AIDS than he did in medical school while trying to understand what the exposure means for his health, and b) the absolutely maddening battle that he, an actual doctor and very knowledgable & capable patient, has with the absurd “system” of American health care that works to bury people in circuitous phone calls, gotta-be-perfect paperwork, and pass-the-buck bureaucracy to avoid providing necessary medical care. The phone call with the pharmacist at the 27:05 mark would be the height of absurdist humor if it weren’t so infuriating.
If an actual health care professional had to work this hard to get what he needed, what are the chances that someone without his level of knowledge, time, and resources is going to be able to? This whole extractive, regressive system needs to fucking go. (thx, matt)
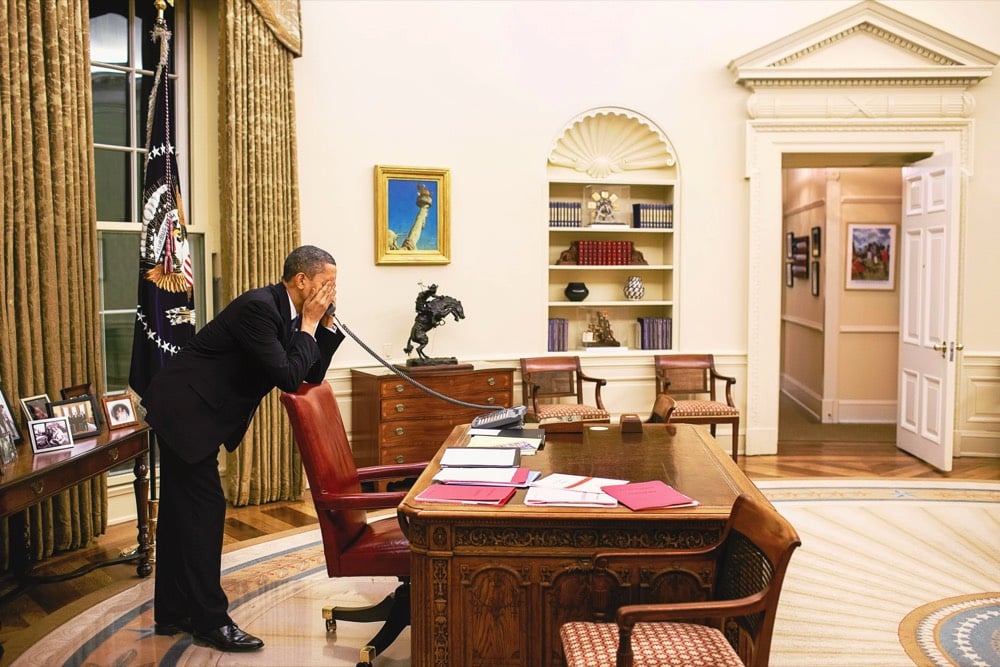
Barack Obama’s forthcoming memoir, A Promised Land, is coming out next month. The New Yorker is running an excerpt of the book, an account of his administration’s struggle to get the Affordable Care Act through Congress.
As time went on, though, it became hard to ignore some of the more troubling impulses driving the movement. As had been true at Palin rallies, reporters at Tea Party events caught attendees comparing me to animals or Hitler. Signs turned up showing me dressed like an African witch doctor with a bone through my nose. Conspiracy theories abounded: that my health-care bill would set up “death panels” to evaluate whether people deserved treatment, clearing the way for “government-encouraged euthanasia,” or that it would benefit illegal immigrants, in the service of my larger goal of flooding the country with welfare-dependent, reliably Democratic voters. The Tea Party also resurrected an old rumor from the campaign: that I was not only Muslim but had actually been born in Kenya, and was therefore constitutionally barred from serving as President. By September, the question of how much nativism and racism explained the Tea Party’s rise had become a major topic of debate on the cable shows-especially after the former President and lifelong Southerner Jimmy Carter offered up the opinion that the extreme vitriol directed toward me was at least in part spawned by racist views.
At the White House, we made a point of not commenting on any of this — and not just because Axe had reams of data telling us that white voters, including many who supported me, reacted poorly to lectures about race. As a matter of principle, I didn’t believe a President should ever publicly whine about criticism from voters — it’s what you signed up for in taking the job — and I was quick to remind both reporters and friends that my white predecessors had all endured their share of vicious personal attacks and obstructionism.
More practically, I saw no way to sort out people’s motives, especially given that racial attitudes were woven into every aspect of our nation’s history. Did that Tea Party member support “states’ rights” because he genuinely thought it was the best way to promote liberty, or because he continued to resent how federal intervention had led to desegregation and rising Black political power in the South? Did that conservative activist oppose any expansion of the social-welfare state because she believed it sapped individual initiative or because she was convinced that it would benefit only brown people who had just crossed the border? Whatever my instincts might tell me, whatever truths the history books might suggest, I knew I wasn’t going to win over any voters by labelling my opponents racist.
The harbingers of Trumpism throughout this piece are difficult to ignore.
In a his book out today, Which Country Has the World’s Best Health Care?, oncologist & bioethicist Ezekiel Emanuel compares the outcomes of several countries’ health care systems.
The US spends more than any other nation, nearly $4 trillion, on healthcare. Yet, for all that expense, the US is not ranked #1 — not even close.
In Which Country Has the World’s Best Healthcare? Ezekiel Emanuel profiles 11 of the world’s healthcare systems in pursuit of the best or at least where excellence can be found. Using a unique comparative structure, the book allows healthcare professionals, patients, and policymakers alike to know which systems perform well, and why, and which face endemic problems. From Taiwan to Germany, Australia to Switzerland, the most inventive healthcare providers tackle a global set of challenges — in pursuit of the best healthcare in the world.
In his ranking of 11 countries profiled, China and the United States are, respectively, dead last and second-to-last in providing health care for their citizens. In the case of the United States at least, that failure is on display with our response to the Covid-19 pandemic.
If you didn’t have the opportunity yesterday to watch Jon Stewart’s scathing and powerful opening statement before a House subcommittee about providing health benefits for surviving 9/11 first responders, you really should; it’s quite something:
As I sit here today, I can’t help but think what an incredible metaphor this room is for the entire process that getting healthcare and benefits for 9/11 first responders has come to. Behind me, a filled room of 9/11 first responders and in front of me a nearly empty Congress.
Shameful. It’s an embarrassment to the country and it is a stain on this institution. You should be ashamed of yourselves, for those that aren’t here, but you won’t be. Because accountability doesn’t appear to be something that occurs in this chamber.
On Twitter, archivist Jason Scott shared a cache of over 2300 photos taken by a worker at Ground Zero during the cleanup process in September & October 2001. These photos provide a unique and documentary view of the work being done there, work on behalf of Americans everywhere that this worker, and many others, paid for with his life. Scott:
So, it would probably be useful to interview the worker who took all these photos, who walked around the grounds, who captured these unique images of Ground Zero from all over the space, showing the effort being done to clear the wreckage.
Except we can’t.
He’s dead.


The parallels of all this to HBO’s Chernobyl miniseries is left as an exercise to the reader.
Update: The House subcommittee approved extending the compensation fund for 9/11 first responders until 2090. The bill is expected to pass a full House vote but the Senate is anyone (but Mitch McConnell’s) guess.
Update: For his efforts, one of the first responders gifted Stewart a firefighter’s jacket that belonged to a good friend of his, now deceased:
This story on the merger of two eyeglass giants, Essilor (“a French multinational that controls almost half of the world’s prescription lens business and has acquired more than 250 other companies in the past 20 years”) and Luxottica (“an Italian company with an unparalleled combination of factories, designer labels and retail outlets,” including Ray-Ban and LensCrafters) also contains this appraisal of the state of vision across the globe:
No one is exactly sure what it is about early 21st-century urban living - the time we spend indoors, the screens, the colour spectrum in LED lighting, or the needs of ageing populations - but the net result is that across the world, we are becoming a species wearing lenses. The need varies depending where you go, because different populations have different genetic predispositions to poor eyesight, but it is there, and growing, and probably greater than you think. In Nigeria, around 90 million people, or half the population, are now thought to need corrective eyewear…. An estimated 2.5 billion people, mostly in India, Africa and China, are thought to need spectacles, but have no means to have their eyes tested or to buy them.
“Eye-health campaigners call it the largest untreated disability in the world,” says the author. “It is also a staggering business opportunity.”
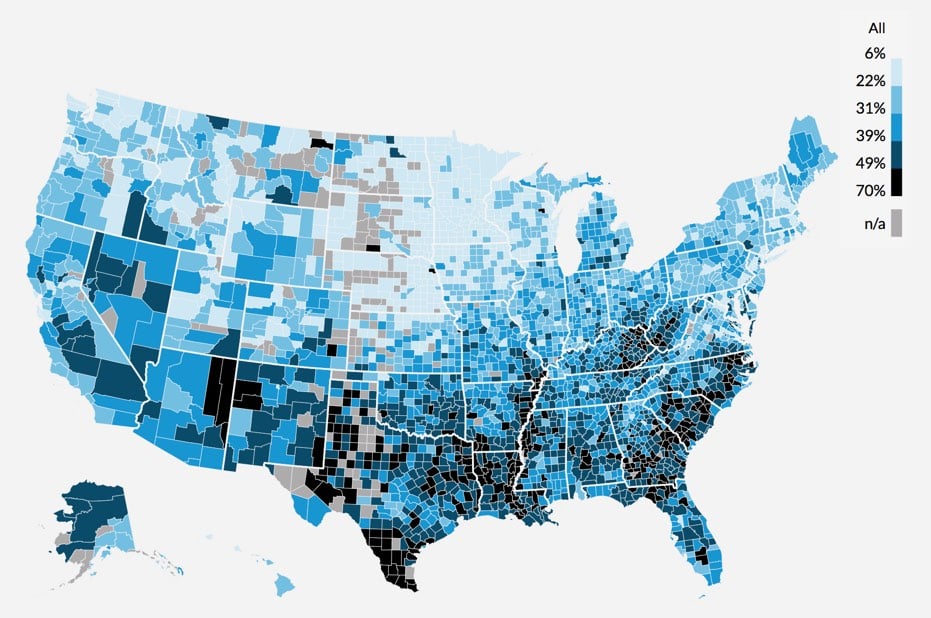
The Urban Institute has built an interactive map for exploring debt in America.
Credit can be a lifeline during emergencies and a bridge to education and homeownership. But debt-which can stem from credit or unpaid bills-often burdens families and communities and exacerbates wealth inequality. This map shows the geography of debt in America at the national, state, and county levels.
I’d love to hear why the “share with any debt in collections” is so relatively low in the Upper Midwest, Minnesota in particular.
Update: Unsurprisingly, health insurance coverage is a significant factor in American debt…and Minnesota has a low rate of medical debt in collections along with a relatively low rate of uninsured. This 2016 press release from MN Department of Health provides some clues as to why the uninsured rate is so comparatively low. (via @yodaui)
Arizona Senator John McCain has publicly come out against the latest Republican attempt to repeal the ACA. His statement begins:
As I have repeatedly stressed, health care reform legislation ought to be the product of regular order in the Senate. Committees of jurisdiction should mark up legislation with input from all committee members, and send their bill to the floor for debate and amendment. That is the only way we might achieve bipartisan consensus on lasting reform, without which a policy that affects one-fifth of our economy and every single American family will be subject to reversal with every change of administration and congressional majority.
I would consider supporting legislation similar to that offered by my friends Senators Graham and Cassidy were it the product of extensive hearings, debate and amendment. But that has not been the case. Instead, the specter of September 30th budget reconciliation deadline has hung over this entire process.
Many opponents of the ACA repeal are hailing McCain as a hero for going against his party leadership on this issue. I don’t see it — he’d still support a bill like Graham-Cassidy that would take away healthcare coverage from millions of Americans if only it were the result of proper procedure — particularly because of what he says next (italics mine):
We should not be content to pass health care legislation on a party-line basis, as Democrats did when they rammed Obamacare through Congress in 2009.
This is false. The NY Times’ David Leonhardt explained back in March during another Republican repeal effort:
When Barack Obama ran for president, he faced a choice. He could continue moving the party to the center or tack back to the left. The second option would have focused on government programs, like expanding Medicare to start at age 55. But Obama and his team thought a plan that mixed government and markets — farther to the right of Clinton’s — could cover millions of people and had a realistic chance of passing.
They embarked on a bipartisan approach. They borrowed from Mitt Romney’s plan in Massachusetts, gave a big role to a bipartisan Senate working group, incorporated conservative ideas and won initial support from some Republicans. The bill also won over groups that had long blocked reform, like the American Medical Association.
But congressional Republicans ultimately decided that opposing any bill, regardless of its substance, was in their political interest. The consultant Frank Luntz wrote an influential memo in 2009 advising Republicans to talk positively about “reform” while also opposing actual solutions. McConnell, the Senate leader, persuaded his colleagues that they could make Obama look bad by denying him bipartisan cover.
Adam Jentleson, former Deputy Chief of Staff for Senator Harry Reid, said basically the same thing on Twitter:
The votes were party-line, but that was a front manufactured by McConnell. He bragged about it at the time. McConnell rarely gives much away but he let the mask slip here, saying he planned to oppose Obamacare regardless of what was in the bill. Those who worked on and covered the bill know there were GOP senators who wanted to support ACA — but McConnell twisted their arms. On Obamacare, Democrats spent months holding hearings and seeking GOP input — we accepted 200+ GOP amendments!
For reference, here was the Senate vote, straight down party lines. Hence the “ramming” charge…if you didn’t know any better. Luckily, Snopes does know better.
According to Mark Peterson, chair of the UCLA Department of Public Policy, one easy metric by which to judge transparency is the number of hearings held during the development of a bill, as well as the different voices heard during those hearings. So far, the GOP repeal efforts have been subject to zero public hearings.
In contrast, the ACA was debated in three House committees and two Senate committees, and subject to hours of bipartisan debate that allowed for the introduction of amendments. Peterson told us in an e-mail that he “can’t recall any major piece of legislation that was completely devoid of public forums of any kind, and that were crafted outside of the normal committee and subcommittee structure to this extent”.
The Wikipedia page about the ACA tells much the same story.
Senator John McCain has been diagnosed with a particularly aggressive form of brain cancer. The tumor has been removed and McCain is recovering at home with his family. I wish Senator McCain well and hope for a speedy recovery.
In the wake of his diagnosis, many of those expressing support for McCain reference his considerable personal strength in his fight against cancer. President Obama said:
John McCain is an American hero & one of the bravest fighters I’ve ever known. Cancer doesn’t know what it’s up against. Give it hell, John.
McCain’s daughter Meghan references his toughness and fearlessness in a statement released yesterday. Vice-President Joe Biden expressed similar sentiments on Twitter:
John and I have been friends for 40 years. He’s gotten through so much difficulty with so much grace. He is strong — and he will beat this.
This is the right thing to say to those going through something like this, and hearing this encouragement and having the will & energy to meet this challenge will undoubtably increase McCain’s chances of survival. But what Biden said next is perhaps more relevant:
Incredible progress in cancer research and treatment in just the last year offers new promise and new hope. You can win this fight, John.
As with polio, smallpox, measles, and countless other diseases before it, beating cancer is not something an individual can do. Being afflicted with cancer is the individual’s burden to bear but society’s responsibility to cure. In his excellent biography of cancer from 2011, The Emperor of All Maladies, Siddhartha Mukherjee talks about the progress we’ve made on cancer:
Incremental advances can add up to transformative changes. In 2005, an avalanche of papers cascading through the scientific literature converged on a remarkably consistent message — the national physiognomy of cancer had subtly but fundamentally changed. The mortality for nearly every major form of cancer — lung, breast, colon, and prostate — had continuously dropped for fifteen straight years. There had been no single, drastic turn but rather a steady and powerful attrition: mortality had declined by about 1 percent every year. The rate might sound modest, but its cumulative effect was remarkable: between 1990 and 2005, the cancer-specific death rate had dropped nearly 15 percent, a decline unprecedented in the history of the disease. The empire of cancer was still indubitably vast — more than half a million American men and women died of cancer in 2005 — but it was losing power, fraying at its borders.
What precipitated this steady decline? There was no single answer but rather a multitude. For lung cancer, the driver of decline was primarily prevention — a slow attrition in smoking sparked off by the Doll-Hill and Wynder-Graham studies, fueled by the surgeon general’s report, and brought to its full boil by a combination of political activism (the FTC action on warning labels), inventive litigation (the Banzhaf and Cipollone cases), medical advocacy, and countermarketing (the antitobacco advertisements). For colon and cervical cancer, the declines were almost certainly due to the successes of secondary prevention — cancer screening. Colon cancers were detected at earlier and earlier stages in their evolution, often in the premalignant state, and treated with relatively minor surgeries. Cervical cancer screening using Papanicolaou’s smearing technique was being offered at primary-care centers throughout the nation, and as with colon cancer, premalignant lesions were excised using relatively minor surgeries. For leukemia, lymphoma, and testicular cancer, in contrast, the declining numbers reflected the successes of chemotherapeutic treatment. In childhood ALL, cure rates of 80 percent were routinely being achieved. Hodgkin’s disease was similarly curable, and so, too, were some large-cell aggressive lymphomas. Indeed, for Hodgkin’s disease, testicular cancer, and childhood leukemias, the burning question was not how much chemotherapy was curative, but how little: trials were addressing whether milder and less toxic doses of drugs, scaled back from the original protocols, could achieve equivalent cure rates.
Perhaps most symbolically, the decline in breast cancer mortality epitomized the cumulative and collaborative nature of these victories — and the importance of attacking cancer using multiple independent prongs. Between 1990 and 2005, breast cancer mortality had dwindled an unprecedented 24 percent. Three interventions had potentially driven down the breast cancer death rate-mammography (screening to catch early breast cancer and thereby prevent invasive breast cancer), surgery, and adjuvant chemotherapy (chemotherapy after surgery to remove remnant cancer cells).
Understanding how to defeat cancer is an instance where America’s fierce insistence on individualism does us a disservice. Individuals with freedom to pursue their own goals are capable of a great deal, but some problems require massive collective coordination and effort. Beating cancer is a team sport; it can only be defeated by a diverse collection of people and institutions working hard toward the same goal. It will take government-funded research, privately funded research, a strong educational system, philanthropy, and government agencies from around the world working together. This effort also requires a system of healthcare that’s available to everybody, not just to those who can afford it. Although cancer is not a contagious disease like measles or smallpox, the diagnosis and treatment of each and every case brings us closer to understanding how to defeat it. We make this effort together, we spend this time, energy, and money, so that 10, 20, or 30 years from now, our children and grandchildren won’t have to suffer like our friends and family do now.
According to a recent poll, over a third of those polled did not know that Obamacare and the Affordable Care Act were the same thing.
In the survey, 35 percent of respondents said either they thought Obamacare and the Affordable Care Act were different policies (17 percent) or didn’t know if they were the same or different (18 percent). This confusion was more pronounced among people 18 to 29 and those who earn less than $50,000 — two groups that could be significantly affected by repeal.
And that’s perhaps not even the worse part:
For instance, only 61 percent of adults knew that many people would lose coverage through Medicaid or subsidies for private health insurance if the A.C.A. were repealed and no replacement enacted. In contrast, approximately one in six Americans, or 16 percent, said that “coverage through Medicaid and subsidies that help people buy private health insurance would not be affected” by repeal, and 23 percent did not know.
I’ve never liked the Obamacare moniker, but clearly that’s only part of the problem.
I posted earlier about Atul Gawande’s piece in the New Yorker on the importance of incremental care in medicine. One of the things that the Affordable Care Act1 did was to make it illegal for insurance companies to deny coverage to people with “preexisting conditions”, which makes it difficult for those people to receive the type of incremental care Gawande touts. And who has these preexisting conditions? An estimated 27% of US adults under 65, including Gawande’s own son:
In the next few months, the worry is whether Walker and others like him will be able to have health-care coverage of any kind. His heart condition makes him, essentially, uninsurable. Until he’s twenty-six, he can stay on our family policy. But after that? In the work he’s done in his field, he’s had the status of a freelancer. Without the Affordable Care Act’s protections requiring all insurers to provide coverage to people regardless of their health history and at the same price as others their age, he’d be unable to find health insurance. Republican replacement plans threaten to weaken or drop these requirements, and leave no meaningful solution for people like him. And data indicate that twenty-seven per cent of adults under sixty-five are like him, with past health conditions that make them uninsurable without the protections.
That’s 52 million people, potentially ineligible for health insurance. And that’s not counting children. Spurred on by Gawande, people have been sharing their preexisting conditions stories on Twitter with the hashtag #the27Percent.
The 27% figure comes from a recent analysis by the Kaiser Family Foundation:
A new Kaiser Family Foundation analysis finds that 52 million adults under 65 — or 27 percent of that population — have pre-existing health conditions that would likely make them uninsurable if they applied for health coverage under medical underwriting practices that existed in most states before insurance regulation changes made by the Affordable Care Act.
In eleven states, at least three in ten non-elderly adults would have a declinable condition, according to the analysis: West Virginia (36%), Mississippi (34%), Kentucky (33%), Alabama (33%), Arkansas (32%), Tennessee (32%), Oklahoma (31%), Louisiana (30%), Missouri (30%), Indiana (30%) and Kansas (30%).
36% uninsurable in West Virginia! You’ll note that all 11 of those states voted for Trump in the recent election and in West Virginia, Trump carried the day with 68.7% of the vote, the highest percentage of any state. The states whose people need the ACA’s protection the most voted most heavily against their own interest.
Update: An earlier version of this post unfairly pinned the entire blame for the lack of coverage of those with preexisting conditions on the insurance companies.2 I removed the last paragraph because it was more or less completely wrong. Except for the part where I said we should be pissed at the Republican dickheads in Congress who want to repeal the ACA without replacing it with something better.3 And the part where we should be outraged. And the part where we regulated cars and cigarettes and food to make them safer, forced companies to build products in ways they didn’t want, and saved millions of lives. We can’t make everyone healthier and raise taxes to do it? Pathetic for what is supposedly the world’s most powerful and wealthy nation. (thx @JPVMan + many others)
In a piece called The Heroism of Incremental Care for the New Yorker, surgeon Atul Gawande argues that our healthcare system is built for and celebrates heroic intensive care over the slower but more effective efforts of long-term primary care givers.
We have a certain heroic expectation of how medicine works. Following the Second World War, penicillin and then a raft of other antibiotics cured the scourge of bacterial diseases that it had been thought only God could touch. New vaccines routed polio, diphtheria, rubella, and measles. Surgeons opened the heart, transplanted organs, and removed once inoperable tumors. Heart attacks could be stopped; cancers could be cured. A single generation experienced a transformation in the treatment of human illness as no generation had before. It was like discovering that water could put out fire. We built our health-care system, accordingly, to deploy firefighters. Doctors became saviors.
But the model wasn’t quite right. If an illness is a fire, many of them require months or years to extinguish, or can be reduced only to a low-level smolder. The treatments may have side effects and complications that require yet more attention. Chronic illness has become commonplace, and we have been poorly prepared to deal with it. Much of what ails us requires a more patient kind of skill.
Steven Brill has written a book about the making of the Affordable Care Act called America’s Bitter Pill: Money, Politics, Backroom Deals, and the Fight to Fix Our Broken Healthcare System.
America’s Bitter Pill is Steven Brill’s much-anticipated, sweeping narrative of how the Affordable Care Act, or Obamacare, was written, how it is being implemented, and, most important, how it is changing — and failing to change — the rampant abuses in the healthcare industry. Brill probed the depths of our nation’s healthcare crisis in his trailblazing Time magazine Special Report, which won the 2014 National Magazine Award for Public Interest. Now he broadens his lens and delves deeper, pulling no punches and taking no prisoners.
Malcolm Gladwell has a review in the New Yorker this week.
Brill’s intention is to point out how and why Obamacare fell short of true reform. It did heroic work in broadening coverage and redistributing wealth from the haves to the have-nots. But, Brill says, it didn’t really restrain costs. It left incentives fundamentally misaligned. We needed major surgery. What we got was a Band-Aid.
I haven’t read his book yet, but I agree with Brill on one thing: the ACA1 did not go nearly far enough. Healthcare and health insurance are still a huge pain in the ass and still too expensive. My issues with healthcare particular to my situation are:
- As someone who is self-employed, insurance for me and my family is absurdly expensive. After the ACA was enacted, my insurance cost went up and the level of coverage went down. I’ve thought seriously about quitting my site and getting an actual job just to get good and affordable healthcare coverage.
- Doctors aren’t required to take any particular health insurance. So when I switched plans, as I had to when the ACA was enacted, finding insurance that fit our family’s particular set of doctors (regular docs, pediatrician, pediatric specialist that one of the kids has been seeing for a couple of years, OB/GYN, etc.) was almost impossible. We basically had one plan choice (not even through the ACA marketplace…see next item) or we had to start from scratch with new doctors.
- Many doctors don’t take the ACA plans. My doctor doesn’t take any of them and my kids’ doc only took a couple. And they’re explicit in accepting, say, United Healthcare’s regular plan but not their ACA plan, which underneath the hood is the exact same plan that costs the same and has the same benefits. It’s madness.
- The entire process is designed to be confusing so that insurance companies (and hospitals probably too) can make more money. I am an educated adult whose job is to read things so they make enough sense to tell others about them. That’s what I spend 8+ hours a day doing. And it took me weeks to get up to speed on all the options and pitfalls and gotchas of health insurance…and I still don’t know a whole lot about it. It is the most un-user-friendly thing I have ever encountered.
The ACA did do some great things, like making everyone eligible for health insurance and getting rid of the preexisting conditions bullshit, and that is fantastic…the “heroic work” mentioned by Gladwell. But the American healthcare system is still an absolute shambling embarrassment when you compare it to other countries around the world, even those in so-called “developing” or “third world” countries. And our political system is just not up to developing a proper plan, so I guess we’ll all just limp along as we have been. Guh.
According to an article in The Journal of the American Medical Association, the obesity rate of American 2- to 5-year-old children has dropped from 14% in 2004 to 8% in 2012.
Children now consume fewer calories from sugary beverages than they did in 1999. More women are breast-feeding, which can lead to a healthier range of weight gain for young children. Federal researchers have also chronicled a drop in overall calories for children in the past decade, down by 7 percent for boys and 4 percent for girls, but health experts said those declines were too small to make much difference.
Barry M. Popkin, a researcher at the University of North Carolina at Chapel Hill who has tracked American food purchases in a large data project, said families with children had been buying lower-calorie foods over the past decade, a pattern he said was unrelated to the economic downturn.
He credited those habits, and changes in the federally funded Special Supplemental Nutrition Program for Women, Infants and Children, for the decline in obesity among young children. The program, which subsidizes food for low-income women, reduced funding for fruit juices, cheese and eggs and increased it for whole fruits and vegetables.
Kevin Drum calls the drop “baffling”.
Sandra Fluke writes that the portion of Affordable Care Act that guarantees women access to preventative health services went into effect today.
Women across the country have reason to celebrate tonight. Why? Because on Wednesday, the law that provides American women with access to preventive health services, including birth control, at no cost-no co-pay, no increase in premium, no deductible-goes into effect.
Under the law, women are guaranteed “a free annual well-woman visit” (including screenings for domestic violence and HIV), DNA screenings for HPV every three years, free screenings for gestational diabetes for pregnant women, and no-cost contraception. Sometimes it almost feels like we’re not living in the Stone Age here in the US. Almost:
But they do need to find out when their next insurance plan year begins, and make sure their plan qualifies. That’s because — with the exception of women who access their insurance through certain religiously-affiliated non-profits and schools, who unfortunately must wait another year for contraception coverage — this policy takes effect August 1. But each woman’s insurance plan will implement these benefits with the next new plan year after today. So if a woman’s insurance plan year begins on September 15, she’s eligible for these services beginning September 15.
You may not believe me, but this postmortem by SCOTUSblog’s Tom Goldstein of how the media covered the Supreme Court’s decision regarding the Patient Protection and Affordable Care Act is super fascinating. It’s impeccably sourced, straighforward, and surprisingly compelling.
The Court’s own technical staff prepares to load the opinion on to the Court’s website. In years past, the Court would have emailed copies of the decision to the Solicitor General and the parties’ lawyers once it was announced. But now it relies only on its website, where opinions are released approximately two minutes later. The week before, the Court declined our request that it distribute this opinion to the press by email; it has complete faith in the exceptional effort it has made to ensure that the website will not fail.
But it does. At this moment, the website is the subject of perhaps greater demand than any other site on the Internet — ever. It is the one and only place where anyone in the country not at the building — including not just the public, but press editors and the White House — can get the ruling. And millions of people are now on the site anxiously looking for the decision. They multiply the burden of their individual visits many times over — hitting refresh again, and again, and again. In the face of the crushing demand, the Court cannot publish its own decision.
The opinion will not appear on the website for a half-hour. So everyone in the country not personally at 1 First St., NE in Washington, DC is completely dependent on the press to get the decision right.
Reading it, the thing that struck me most is that these huge media machines still operate mostly on an individual basis. One person read the ruling for CNN, told one person in the control room, and then millions and millions of people heard that (mis)information just a few seconds later on CNN, on Twitter, and even in the Oval Office.
I’m surprised and mostly pleased that the Supreme Court has upheld President Obama’s Patient Protection and Affordable Care Act.
The Court’s ruling means, that unless Congress acts, in 2014 all Americans will be required to purchase health insurance in the most sweeping overhaul of the nation’s health care system since the Great Society. The Court, according to early analysis, redefined the mandate as a tax, skirting some Constitutional questions but offering a dramatic affirmation to Obama’s key initiative.
Update: Josh Marshall speaks for me here.
This is an imperfect law. But what’s most important is that it provides a structure under which the country can make a start not only on universal coverage — as an ethical imperative — but on doing away with the waste and inefficiencies created by the chronic market failure of the US health insurance system. Again, that matters. And I suspect that there’s no going back.
Before he died last year at the age of 44, Mike DeStefano shared the story of his wife’s final days many years earlier. She’s in hospice care, DeStefano shows up with his new Harley and takes her for a ride, morphine drip and all.
She’s holding the pole [of the IV drip]! Marc, it was a pole with four wheels on the bottom, and we’re riding around this hospice, and you could hear the goddamn wheels jangling and banging; it was insane.
And then I pass the front door, and all these nurses are standing out front, and they’re all crying. They’re watching us, and they’re crying. And I didn’t know why they were crying. I was like, Why are they crying? I didn’t get what they were seeing. I didn’t know. Because I was just in it; I was living it. I knew my wife who had suffered, she was a prostitute, she was a freakin’ heroin addict, she was beaten by pimps — this was her past — and then she ends up with AIDS, and she’s dying, and all she wants is a goddamn ride on my motorcycle.
So the next thing you know we’re on I-95, because women, it’s never enough for them. We’re on I-95, and she unhooks the pole, and she’s holding the morphine bag over her head with her gown that’s flying up in the air so you could see her entire naked, bony body with the morphine bag whipping in the wind, and we’re passing by these guys in their Lamborghinis, and I’m looking at them like, What the hell kind of life are you living? Look at me, I’m on top of the world here.
I love this story. The podcast from which it was taken is available here.
Older posts
Socials & More