kottke.org posts about Covid-19
A few weeks ago, writer Kyle Chayka Tweeted “I predict a great Blogging Renaissance,” to which also writer Kevin Nguyen responded, “i kinda wanna do a weird free-for-all quarantine blog.” Then they added other writer Bijan Stephen and started Indoor Voices, a group blog which has now grown to about 80 members, all of whom miss what the internet used to be like AND happen to be home quite a bit at the moment. (To cement old school credentials, Indoor Voices is hosted on ancient blogging platform Blogspot, the place I got my blogging start in 2004. (Out of an abundance of shame, I absolutely will not be linking to this first blog.))
From the Indoor Voices about page:
Blogging is not a substitute for direct action. Direct action in this case involves staying home. Blogging is one thing to do while staying at home. Please wash your hands. It’s hard to believe, but there was a time where the internet was just full of casual websites posting random stuff. And you’d go to them maybe even multiple times a day to see if they had posted any new stories. It was something we all did when we were bored at our desks, at our jobs. Now there are no more desks. But there are still blogs.
There’s no theme, except quarantine. There’s no schedule, except people post every day whenever they want. As you might expect from a group of 80 people, post subjects vary. There are beauty tips, missives to Deadwood and Steven Universe, strategies to get through your pile of New Yorkers, and a regularly featured What Should You Do Tonight? I myself have posted about working from home with kids (it’s…fine), what help small businesses need right now, and Quarantine, an anthem sung to the tune of Dolly Parton’s, Jolene. (This level of blogging productivity hasn’t been seen by me since 2014.)
In a brief interview, cofounder Kevin Nguyen had this to say about Indoor Voices:
We started Indoor Voices because we were nostalgic for classic days of blogging, and partly as an inside joke. Then we realized that the blogs we missed felt like an inside joke that a small community was in on. So far, we’ve been really thrilled with the creative, chaotic energy that people have been putting forward. It’s writing for writing’s sake, and we’ve enjoyed seeing just how diverse and funny and strange that’s been. Probably helps that we’re all slowly going stir crazy.
Note also, Kevin’s first novel, New Waves, is finally out. It’s my most anticipated read of the year, but don’t take my word for it. Almost every publication that writes about books regularly listed it as anticipated as well.
Note: Please check the updates below for some important corrections to some of the information in this video.
From Dr. Jeffrey VanWingen MD, a video on how to ensure that your grocery shopping experience is as safe as possible and to avoid potential COVID-19 infection from plastic and metal surfaces. I’m going to be honest with you: a lot of this seems like overkill (as it should — see the Paradox of Preparation). However, this is also pretty much what I’ve been doing after grocery shopping for the past 2 weeks because I am a fastidious motherfucker1 with plenty of time to wipe down groceries. If it comes down to a choice between watching 7 more minutes of The Mandalorian or wiping down my groceries before putting them in the fridge, I’m gonna wipe them groceries. Baby Yoda can wait.
See also this PDF from Crumpton Group about how to keep your household free of the outside effects of the COVID-19 pandemic.
Household members should understand that their principal effort should be directed towards isolating the inside of the home from the pandemic effects outside. All physical thresholds of the home will serve as a cordon sanitaire. Strive to decontaminate everyone and everything to the best practical degree before entering.
Many of Dr. VanWingen’s recommendations mirror those in the PDF. See also expert guidance on COVID-19 and food safety. (thx, meg)
Update: I have not had a chance to read it yet (was attending to some other things this evening — family, trying to have some normalcy), but I’ve been told that this thread is a good response to the video above. I’ll have a closer look at it tomorrow.
Update: Ok, I’ve read Don Schaffner’s thread criticizing this video. At least I think this is the video he’s referring to because he never says it outright — which I’ll get to in a minute. (Schaffner is a professor in the food science department at Rutgers who I linked to the other day in my post on COVID-19 and food safety.) As he notes, there are a couple of factual errors and VanWingen does offer some dubious advice, particularly about washing food with soap (which I didn’t take seriously). I do not believe, however, that VanWingen was suggesting that people leave frozen items and perishables in a warm garage for 3 days and that the normal rules of food safety are somehow countermanded by potential coronavirus contamination. If you want to leave that box of Cheerios that you don’t need in the car for 3 days, go right ahead. He definitely should have been clearer on that point though.
But the bulk of VanWingen’s video was about how to handle your groceries and takeout food coming into your house to minimize the chance of infection. (And as I mentioned, much of it mirrors the advice in this document and in Dr. Michael Lin’s document from a couple of weeks ago — this isn’t just his opinon or my opinion.) If we are to take seriously a) the assumption that anyone could have COVID-19 (including yourself & grocery workers) that we are operating under w/r/t to handwashing & keeping a 6-foot distance, b) the preliminary results that suggest that SARS-CoV-2 can last on some surfaces for days, and c) that person-to-surface-to-person transfer of SARS-CoV-2 might result in infection (i.e. the reason we are doing all this handwashing and face not-touching), then we should be disinfecting surfaces that other people have been touching recently. Right? We should assume that all surfaces are contaminated. This doesn’t seem outlandish, especially when grocery stores are restocking shelves continuously — that bag of chips that you put into your cart may have been placed on the shelf only 30 minutes before. How is disinfecting your Oreos package when you get home from the store a bad idea? Sure, wash your hands before you eat, but if you have kids, you know how futile that can be sometimes, especially when Oreos are involved. So why not just clean the package? Ditto with transferring takeout food to new containers and giving it a blast in the microwave to warm it up.
Schaffner’s stance is that most surfaces aren’t contaminated to a high degree, which is undoubtably true. Having watched the video & read Schaffner’s advice (and other advice by other experts), where your personal comfort level with making sure the surfaces you and your family come into contact to are disinfected is up to you. Ultimately, advice from experts is still advice and you have to figure out whether it works for you. It’s easy to believe you should wash your hands frequently because that’s universal advice. But “you should disinfect surfaces you touch” and “you don’t have to worry too much about disinfecting your grocery packages” are genuinely conflicting bits of advice from well-meaning experts! You’ve gotta use your noggin and make up your own mind, based on your personal idea of risk and safety. It’s gonna land differently with different people.
Finally, I’m going to get a little cranky here, but I found Schaffner’s overall tone in the first few tweets of that thread mocking, ungenerous, and unhelpful. Instead of gently offering alternative authoritative advice, he subtweeted (by refusing to link to the video and calling Dr. VanWingen not by his name but referring to him as “the video MD”) and made fun of VanWingen’s outfit. I know it must be frustrating to see what you perceive as misinformation out there, but we do not need Doctor vs Doctor battles here. Everyone’s just going to get defensive and dig their heels in.
Update: From Joseph Allen of Harvard’s School of Public Health, Don’t panic about shopping, getting delivery or accepting packages.
Yes, the virus can be detected on some surfaces for up to a day, but the reality is that the levels drop off quickly. For example, the article shows that the virus’s half-life on stainless steel and plastic was 5.6 hours and 6.8 hours, respectively. (Half-life is how long it takes the viral concentration to decrease by half, then half of that half, and so on until it’s gone.)
And here’s how to take reasonable precautions when getting a package delivery or going to the grocery store:
You can leave that cardboard package at your door for a few hours - or bring it inside and leave it right inside your door, then wash your hands again. If you’re still concerned there was any virus on the package, you could wipe down the exterior with a disinfectant, or open it outdoors and put the packaging in the recycling can. (Then wash your hands again.)
What about going to the grocery store? The same approach applies.
Shop when you need to (keeping six feet from other customers) and load items into your cart or basket. Keep your hands away from your face while shopping, and wash them as soon as you’re home. Put away your groceries, and then wash your hands again. If you wait even a few hours before using anything you just purchased, most of the virus that was on any package will be significantly reduced. If you need to use something immediately, and want to take extra precautions, wipe the package down with a disinfectant. Last, wash all fruits and vegetables as you normally would.
Important caveat: the coronavirus half-life times are for room temperature. For colder temperatures (like in the fridge or especially the freezer), the virus will last longer. So maybe wipe down that bag of frozen peas even if you’re not going to use them for a couple of days.
For That Discomfort You’re Feeling Is Grief, HBR’s Scott Berinato interviewed David Kessler, who he calls “the world’s foremost expert on grief”, about what we’re collectively feeling as we deal with the COVID-19 pandemic.
HBR: People are feeling any number of things right now. Is it right to call some of what they’re feeling grief?
Kessler: Yes, and we’re feeling a number of different griefs. We feel the world has changed, and it has. We know this is temporary, but it doesn’t feel that way, and we realize things will be different. Just as going to the airport is forever different from how it was before 9/11, things will change and this is the point at which they changed. The loss of normalcy; the fear of economic toll; the loss of connection. This is hitting us and we’re grieving. Collectively. We are not used to this kind of collective grief in the air.
HBR: You said we’re feeling more than one kind of grief?
Kessler: Yes, we’re also feeling anticipatory grief. Anticipatory grief is that feeling we get about what the future holds when we’re uncertain. Usually it centers on death. We feel it when someone gets a dire diagnosis or when we have the normal thought that we’ll lose a parent someday. Anticipatory grief is also more broadly imagined futures. There is a storm coming. There’s something bad out there. With a virus, this kind of grief is so confusing for people. Our primitive mind knows something bad is happening, but you can’t see it. This breaks our sense of safety. We’re feeling that loss of safety. I don’t think we’ve collectively lost our sense of general safety like this. Individually or as smaller groups, people have felt this. But all together, this is new. We are grieving on a micro and a macro level.
And what can we start to do about our grief?
Understanding the stages of grief is a start. But whenever I talk about the stages of grief, I have to remind people that the stages aren’t linear and may not happen in this order. It’s not a map but it provides some scaffolding for this unknown world. There’s denial, which we say a lot of early on: This virus won’t affect us. There’s anger: You’re making me stay home and taking away my activities. There’s bargaining: Okay, if I social distance for two weeks everything will be better, right? There’s sadness: I don’t know when this will end. And finally there’s acceptance. This is happening; I have to figure out how to proceed.
Acceptance, as you might imagine, is where the power lies. We find control in acceptance. I can wash my hands. I can keep a safe distance. I can learn how to work virtually.
Kessler recently came out with a new book called Finding Meaning: The Sixth Stage of Grief.
I wrote a bit about grief a couple years back in this post How Do You Help a Grieving Friend?
One of the odd things about getting older (and hopefully wiser) is that you stop chuckling at cliches and start to acknowledge their deep truths. A recent example of this for me is “the only way out is through”. As Devine notes, in this video and her book It’s OK That You’re Not OK, there’s no shortcut for dealing with pain…you have to go through it to move past it.
See also a collection of resources for dealing with death compiled by Chrysanthe last year. (via laura olin)
Update: Trouble Focusing? Not Sleeping? You May Be Grieving by novelist R.O. Kwon:
Other people who couldn’t stay home were going to work every day — many without the option, the privilege, of doing otherwise — while here I was, home, and I couldn’t, of all things, write. Yes, there’s a pandemic, and yes, I felt by turns anxious, furious, and terrified, but it’s 2020 in America, and I’ve felt quite anxious, furious and terrified for a while. The inability to work, though, was new.
But then it occurred to me, as I ate another astringent chip, that this lassitude, the trouble focusing, the sleep difficulties, my exhaustion: Oh yes, I thought, I remember this. I was grieving. I was grieving in early March, I’m still grieving now, and chances are, you are, too.
(via @_chrysanthe)
This is a short drone tour of San Francisco with the shelter-in-place order in effect — it looks abandoned. Fisherman’s Wharf, downtown, Market Street, the Haight — I think I saw like 8 people total during the whole video. Heartening to see that people are taking shelter-in-place seriously.
Update: Walking through the empty streets of Rotterdam:
A similar amble through Amsterdam. Here’s NYC:
(via the morning news)
Update: And here’s Miami:
From Ed Yong at the Atlantic, a great article on the current state of the pandemic in the United States, what will happen over the next few months, how it will end, and what the aftermath will be.
With little room to surge during a crisis, America’s health-care system operates on the assumption that unaffected states can help beleaguered ones in an emergency. That ethic works for localized disasters such as hurricanes or wildfires, but not for a pandemic that is now in all 50 states. Cooperation has given way to competition; some worried hospitals have bought out large quantities of supplies, in the way that panicked consumers have bought out toilet paper.
Partly, that’s because the White House is a ghost town of scientific expertise. A pandemic-preparedness office that was part of the National Security Council was dissolved in 2018. On January 28, Luciana Borio, who was part of that team, urged the government to “act now to prevent an American epidemic,” and specifically to work with the private sector to develop fast, easy diagnostic tests. But with the office shuttered, those warnings were published in The Wall Street Journal, rather than spoken into the president’s ear. Instead of springing into action, America sat idle.
Rudderless, blindsided, lethargic, and uncoordinated, America has mishandled the COVID-19 crisis to a substantially worse degree than what every health expert I’ve spoken with had feared. “Much worse,” said Ron Klain, who coordinated the U.S. response to the West African Ebola outbreak in 2014. “Beyond any expectations we had,” said Lauren Sauer, who works on disaster preparedness at Johns Hopkins Medicine. “As an American, I’m horrified,” said Seth Berkley, who heads Gavi, the Vaccine Alliance. “The U.S. may end up with the worst outbreak in the industrialized world.”
If you’ve been reading obsessively about the pandemic, there’s not a lot new in here, but Yong lays the whole situation out very clearly and succinctly (he easily could have gone twice as long). The section on potential after effects was especially interesting:
Pandemics can also catalyze social change. People, businesses, and institutions have been remarkably quick to adopt or call for practices that they might once have dragged their heels on, including working from home, conference-calling to accommodate people with disabilities, proper sick leave, and flexible child-care arrangements. “This is the first time in my lifetime that I’ve heard someone say, ‘Oh, if you’re sick, stay home,’” says Adia Benton, an anthropologist at Northwestern University. Perhaps the nation will learn that preparedness isn’t just about masks, vaccines, and tests, but also about fair labor policies and a stable and equal health-care system. Perhaps it will appreciate that health-care workers and public-health specialists compose America’s social immune system, and that this system has been suppressed.
Aspects of America’s identity may need rethinking after COVID-19. Many of the country’s values have seemed to work against it during the pandemic. Its individualism, exceptionalism, and tendency to equate doing whatever you want with an act of resistance meant that when it came time to save lives and stay indoors, some people flocked to bars and clubs. Having internalized years of anti-terrorism messaging following 9/11, Americans resolved to not live in fear. But SARS-CoV-2 has no interest in their terror, only their cells.
I really hope that Betteridge’s law is wrong about that headline I wrote.

Instructions for staying at home during the pandemic, courtesy of Ikea Israel. (thx, caroline)
When America wants to know how bad things are in a crisis, they look not to the President or FEMA, they look to Waffle House.
The “Waffle House Index,” first coined by Federal Emergency Management Agency Director W. Craig Fugate, is based on the extent of operations and service at the restaurant following a storm and indicates how prepared a business is in case of a natural disaster.
For example, if a Waffle House store is open and offering a full menu, the index is green. If it is open but serving from a limited menu, it’s yellow. When the location has been forced to close, the index is red. Because Waffle House is well prepared for disasters, Kouvelis said, it’s rare for the index to hit red. For example, the Joplin, Mo., Waffle House survived the tornado and remained open.
At last count (as of 10:42am on 3/25), 418 Waffle House restaurants across the country were closed, an unprecedented event. The remainder, from what I can gather from social media and news reports, are operating on a carry-out basis only. Kudos to them for doing the right thing in trying to keep their employees and patrons safe.
Today’s must-read is What I Learned When My Husband Got Sick With Coronavirus by NY Times editor Jessica Lustig. If you’re on the fence about whether COVID-19 is worth all this fuss, Lustig’s account of caring for her gravely ill husband in a Brooklyn apartment while trying to keep herself and their daughter from getting sick should help straighten out your thinking.
Now we live in a world in which I have planned with his doctor which emergency room we should head to if T suddenly gets worse, a world in which I am suddenly afraid we won’t have enough of the few things tempering the raging fever and soaking sweats and severe aches wracking him — the Advil and Tylenol that the doctors advise us to layer, one after the other, and that I scroll through websites searching for, seeing “out of stock” again and again. We are living inside the news stories of testing, quarantine, shortages and the disease’s progression. A friend scours the nearby stores and drops off a bunch of bodega packets of Tylenol. Another finds a bottle at a more remote pharmacy and drops it off, a golden prize I treasure against the feverish nights to come.
His doctor calls three days later to say the test is positive. I find T lying on his side, reading an article about the surge in confirmed cases in New York State. He is reading stories of people being hospitalized, people being put on ventilators to breathe, people dying, sick with the same virus that is attacking him from the inside now.
This is a rough read, no doubt about it. I started crying at the part about his father’s sweater.
Like many of you, I’ve been wondering about COVID-19 & food safety. Is it safe to eat takeout prepared by your local restaurant? To answer that and many other questions, Kenji Lopez-Alt has compiled a comprehensive guide to food safety and coronavirus for Serious Eats. Kenji is the most fastidious and exacting food person I know — how could you think otherwise after having read The Food Lab? — so I take his thoughts and research on this very seriously.
Even so, plenty of folks — myself included — have been confused or curious about the safety of allowing restaurants to continue preparing and serving food. Is it actually safe? Should I reheat the food when I get it home? Is it better to support local businesses by ordering food, or am I only putting workers and delivery people at risk? And if I’m cooking my own food, what guidelines should I follow?
To answer these questions, I referenced dozens of articles and scientific reports and enlisted the help of Ben Chapman, a food safety specialist from the North Carolina State University and cohost of Risky or Not and Food Safety Talk.
Let’s get right to the nitty gritty:
Q: Can I get COVID-19 from touching or eating contaminated food?
According to multiple health and safety organizations worldwide, including the CDC, the USDA, and the European Food Safety Authority, there is currently no evidence that COVID-19 has spread through food or food packaging. Previous coronavirus epidemics likewise showed no evidence of having been spread through food or packaging.
Be sure to read on for answers to questions like “Are we going to run out of food?” and “Am I more likely to get COVID-19 from take-out, delivery, or cooking at home?”
The FDA has a coronavirus safety page on their website as well.
Unlike foodborne gastrointestinal (GI) viruses like norovirus and hepatitis A that often make people ill through contaminated food, SARS-CoV-2, which causes COVID-19, is a virus that causes respiratory illness. Foodborne exposure to this virus is not known to be a route of transmission.
In a piece from March 14, Amanda Mull talked with epidemiologist Stephen Morse from Columbia University about food safety:
Even if the person preparing it is sick, he told me via email, “cooked foods are unlikely to be a concern unless they get contaminated after cooking.” He granted that “a salad, if someone sneezes on it, might possibly be some risk,” but as long as the food is handled properly, he said, “there should be very little risk.”
And Don Schaffner, a professor in the food science department at Rutgers, has been posting information on food safety & COVID-19 on Twitter.
Even if a sick worker sneezed on my food (I know that’s gross), my risk of contracting COVID-19 from it are very low.
First it’s important to realize that this is a respiratory illness as far as we know. The biggest risk is being around sick people who are shedding the virus when they sneeze or cough.
Even if the virus did get onto food, we’re going to put that food in our mouth and swallow it so the virus will end up in our stomach. Our stomachs have a low pH which would likely in activate the virus.
Hey folks, just wanted to check in on a few things this morning. I hope you are staying healthy and kind.
1. I spent some time this weekend on the Quick Links infrastructure. (Quick Links are posted to the @kottke Twitter acct and displayed on the front page of the site, right under the most recent post.) There is now a public archive of the Quick Links available here. (If you’re a kottke.org member, you’ve had access to this for months now.) I also started periodically pushing the Quick Links into kottke.org’s RSS feed (yes, ppl still use RSS…at least tens of thousands of them by my count).
2. After a hiatus, I have restarted kottke.org’s newsletter. It was previously a weekly affair, but due to quick moving pandemic news and information, I’m now trying to publish a couple times a week at least. Click here to subscribe.
3. If you’re a regular reader, you’ve noticed that about two weeks ago, I abruptly switched to covering the COVID-19 pandemic almost exclusively. Aside from 9/11, kottke.org has never been focused on a single topic like this, but I believed it was important to get the word out about how infectious diseases spread and how seriously we should be taking this. (VERY SERIOUSLY.) I still believe that. But the site will likely start wandering back towards other topics this week, at least a little bit. This crisis is hitting all of us in many different ways — some are sick, some are bored, some are terrified, some are out there on the front lines saving lives. I hope it’s possible to keep all of those folks (and their different realities & needs) in our minds & hearts while still finding moments of connection to other kinds of human interests and obsessions.
Thanks for reading.
Some people feel helpless & anxious.
Some people are bored.
Some people are self-quarantined alone and are lonely.
Some people are realizing that After will be very different from Before.
Some people are really enjoying this extra time with their kids and will miss it when it’s over.
Some people just got off their 12th double shift in a row at the hospital and can’t hug their family.
Some people visited their favorite restaurant for the last time and didn’t realize it.
Some people have died from COVID-19.
Some people can’t stop reading the news.
Some people cannot afford soap.
Some people are learning how to bake bread.
Some people are working from home while simultaneously trying to homeschool their kids.
Some people are single parents trying to work from home while simultaneously trying to homeschool their kids.
Some people are living paycheck to paycheck and the next one will not arrive.
Some people are unfit to be President.
Some people left the city for their home in the country.
Some people can’t go to the grocery store because they’re at risk.
Some people lost their jobs.
Some people can’t sleep.
Some people are watching free opera online.
Some people have been quarantined for weeks.
Some people can’t work remotely.
Some people have contracted COVID-19 and don’t know it yet.
Some people can’t concentrate on their work because of anxiety.
Some people can’t afford their rent next month.
Some people are still gathering in large groups.
Some people are keeping the rest of us alive at significant personal risk.
Some people didn’t buy enough hand sanitizer.
Some people bought too much hand sanitizer.
Some people are missing their therapist.
Some people can’t go to work but are still being paid by their employers. For now.
Some people are mainly concerned about what to watch next on Netflix.
Some people are volunteering.
Some people are going to lose their business.
Some people are realizing that teachers are amazing.
Some people are ordering takeout from local restaurants.
Some people would really just like a hug.
Some people can’t convince their elderly parents to take this seriously.
Some people are worried about their 401K.
Some people have never had a 401K.
Some people will face increased abuse at home.
Some people are going to get sick or injured and will have a harder time getting medical care.
Some people can’t buy the food they need because the WIC-eligible stuff is sold out.
Some people won’t stop partying.
Some people lost their childcare.
Some people are doing everything they can to remain calm and hopeful and it’s not working.
Some people are watching Outbreak & Contagion and playing Pandemic.
Some people don’t know what they’re going to do.
Some people are overwhelmed with advice on how to work from home.
Some people are drinking or eating too much.
Some people are thinking about after.
Some people are upset because they can’t travel.
Some people are horny.
Some people are planning for a larger garden this year.
Some people won’t see their families for months.
Some people are logging off to stay grounded.
Some people can’t see the light at the end of the tunnel.
Some people will realize they need to split with their partner.
Some people are singing Imagine.
Some people aren’t on this list.
These are all based on the experiences of real people drawn from news stories, social media, and friends. Take heart: you are not the only person experiencing what you are going through. But be mindful: not everyone is having the same experience you are. Ultimately though, we are all in this together.
On March 10, Tomas Pueyo published a widely read and praised article called Coronavirus: Why You Must Act Now. Yesterday, in the wake of the Imperial College paper and the criticism of it, Pueyo has published a second article: Coronavirus: The Hammer and the Dance. I urge you to read it — it’s sobering yet hopeful. A summary:
Strong coronavirus measures today should only last a few weeks, there shouldn’t be a big peak of infections afterwards, and it can all be done for a reasonable cost to society, saving millions of lives along the way. If we don’t take these measures, tens of millions will be infected, many will die, along with anybody else that requires intensive care, because the healthcare system will have collapsed.
As the title indicates, Pueyo and his collaborators are suggesting an approach that combines initial aggressive action followed by a longer period of efficient vigilance. First comes the Hammer — we use aggressive measures for weeks, giving our healthcare system time to ramp up & scientists time to research the hell out of this thing and for the world’s testing capability to get up to speed.
And then we Dance.
If you hammer the coronavirus, within a few weeks you’ve controlled it and you’re in much better shape to address it. Now comes the longer-term effort to keep this virus contained until there’s a vaccine.
This is probably the single biggest, most important mistake people make when thinking about this stage: they think it will keep them home for months. This is not the case at all. In fact, it is likely that our lives will go back to close to normal.
But, here’s how the Dance works:
How come South Korea, Singapore, Taiwan and Japan have had cases for a long time, in the case of South Korea thousands of them, and yet they’re not locked down home?
In this video, the South Korea Foreign Minister explains how her country did it. It was pretty simple: efficient testing, efficient tracing, travel bans, efficient isolating and efficient quarantining.
That way, most people aren’t locked down, just those who need to be — the sick, the people who have been with those who have gotten sick, etc. Most people can go back to work, back to fairly normal routines.
I call the months-long period between the Hammer and a vaccine the Dance because it won’t be a period during which measures are always the same harsh ones. Some regions will see outbreaks again, others won’t for long periods of time. Depending on how cases evolve, we will need to tighten up social distancing measures or we will be able to release them. That is the dance of R: a dance of measures between getting our lives back on track and spreading the disease, one of economy vs. healthcare.
This piece in the Atlantic, This Is How We Can Beat the Coronavirus by Aaron E. Carroll & Ashish Jha, advocates for essentially the same approach.
We can create a third path. We can decide to meet this challenge head on. It is absolutely within our capacity to do so. We could develop tests that are fast, reliable, and ubiquitous. If we screen everyone, and do so regularly, we can let most people return to a more normal life. We can reopen schools and places where people gather. If we can be assured that the people who congregate aren’t infectious, they can socialize.
We can build health-care facilities that do rapid screening and care for people who are infected, apart from those who are not. This will prevent transmission from one sick person to another in hospitals and other healthcare facilities. We can even commit to housing infected people apart from their healthy family members, to prevent transmission in households.
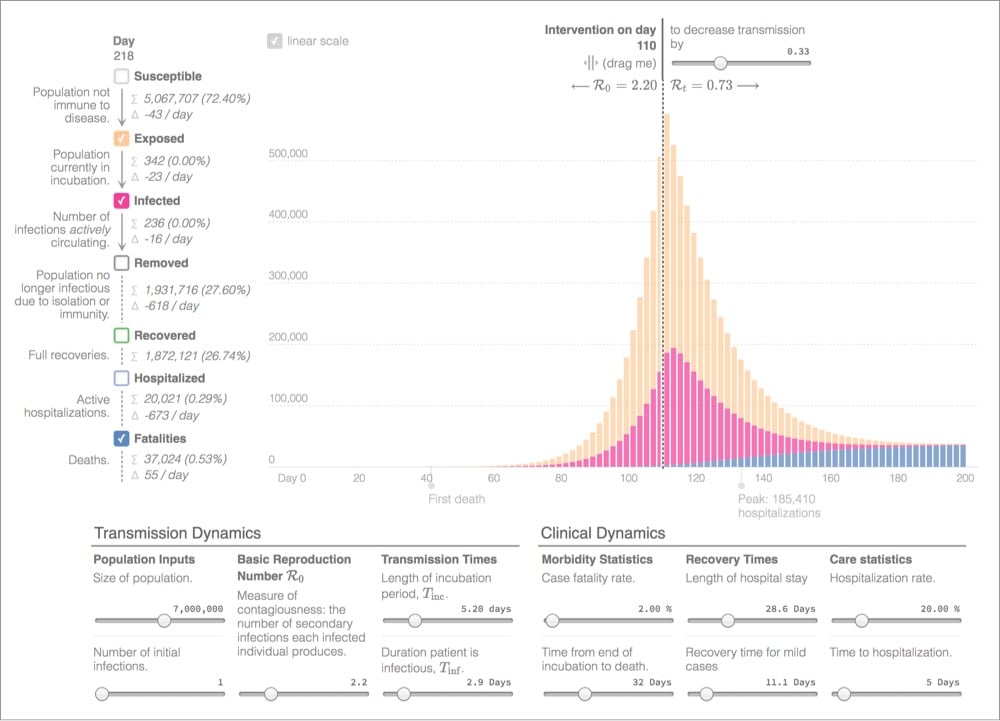
By manipulating values like R0, incubation time, and hospitalization rate with this this epidemic graphing calculator, you really get a sense of how effective early intervention and aggressive measures can be in curbing infection & saving lives in an exponential crisis like the COVID-19 pandemic.
I don’t know if they specifically had this in mind when making it, but this video from Vox about the importance of hand washing with soap to kill coronavirus is very kid-friendly. From my pals at the excellent The Kid Should See This
Wash your hands for 20 seconds with soap and water. This is the very best way to kill viruses like coronavirus. But why? What’s happening on our hands when we use soap and water? And why do we have to wash with soap for 20 seconds? Why not ten?
The glow-in-the-dark explanation of the 20-second rule was extremely convincing.
See also How to Wash Your Hands Properly and Washing Your Hands Is Important Because Soap “Absolutely Annihilates” Coronavirus. (via tksst)
Update: Mark Rober did an experiment with a powder that glows under UV and can be transferred from surface to surface (or hand to surface). You can see the germs spreading from person to person and all over that classroom. Yikes.
This morning Kurzgesagt released their video about COVID-19 that they’ve been working on for a week, and it is excellent, particularly the first part where they explain exactly what the SARS-CoV-2 virus does to a human body and why it can be so dangerous. I hadn’t heard that described before, especially in such relatively simple terms.
The virus has not caused too much damage yet, but corona is now going to release a real beast on you: your own immune system. The immune system, while there to protect you, can actually be pretty dangerous to yourself and needs tight regulation. And as immune cells pour into the lungs to fight the virus, corona infects some of them and creates confusion. Cells have neither ears nor eyes — they communicate mostly via tiny information proteins called cytokines — nearly every important immune reaction is controlled by them. Corona causes infected immune cells to overreact and yell bloody murder. In a sense, it puts the immune system into a fighting frenzy and sends way more soldiers than it should, wasting its resources and causing damage.
Kurzgesagt always provides a list of scientific sources used to produce their videos, and the one for this video is particularly extensive and they are going to keep it updated.
Update: For more information on the coronavirus itself, SARS-CoV-2, see Ed Yong’s piece in the Atlantic and How the Coronavirus Could Take Over Your Body (Before You Ever Feel It) from New York magazine.
One of the key shortages in areas overwhelmed by COVID-19 patients (like Italy) is ventilators in hospitals. COVID-19 is a respiratory illness and respirators are essential in treating patients with acute symptoms. In the US and other countries, experts are warning of ventilator shortages and manufacturers say it will be difficult to ramp up production quickly enough to meet demand. So healthcare providers are looking for other solutions.
One potential solution is modifying ventilators to work for more than one person at a time. Based on feasibility research published in 2006, the simple technique uses inexpensive parts that hospitals already have on hand to modify machines to work with 4 patients at a time (with important caveats). One of the authors of that research paper, Dr. Charlene Babcock, explains how to hack the ventilators in this video:
Some notes from the video:
- The initial study used test lungs (not actual humans)
- You need to make sure the lung size and resistance of all four patients hooked up to a single ventilator are the same. No mixing adults and kids, for instance.
- Make sure the ventilator tubes leading to and from the patients are all the same length.
- This technique has been used successfully in the field, during the aftermath of the 2017 Las Vegas shooting.
- They did not investigate cross-contamination effects, so you have to make sure all the patients connected to one machine are COVID-19 patients in order to mitigate the risk.
In closing, Babcock says:
Now here’s my disclaimer. This is off-label use of the ventilator. The ventilator is made for one person and I’m using it here in a simulation of four patients. I always hope that you would never need to use it in this way, but you can never predict what’s going to happen in a disaster. And if it was me and I had four patients and they all needed intubation and I only had one ventilator, I would simply have a shared discussion meeting with all four families and say “I could pick one to live or we could try to have all four live”. But this is clearly off-label and likely would only be used in dire circumstance, which we may see with COVID-19.
Other people are working on designing and deploying open source ventilators and ventilators made from parts of other machines. All this reminds me of that scene in Apollo 13 where NASA engineers design a modified CO2 scrubber using only parts available on the spacecraft. A similar “failure is not an option” spirit might be called for in this case as well.

Hand sanitizer, a necessary tool in the fight against the COVID-19 pandemic, has been difficult to come by in stores the past few weeks (or months, depending on your location). Last night, I read in a local email newsletter here in Vermont that Mad River Distillers is producing hand sanitizer and giving it away for free to local residents. They’ve set up two pick-up stations for today — it’s BYOB and limited to 6oz per person. Earlier this week, workers at Barr Hill’s closed distillery made hand sanitizer and distributed it to local food shelves. Green Mountain Distillers and Smuggler’s Notch Distillery have also begun producing hand sanitizer.
These Vermont companies join dozens of other distilleries around the country (and world) that have started using high proof alcohol to produce hand sanitizer that meets the CDC’s recommendation of 60% ethanol needed to inactivate the virus that causes COVID-19: Texas, Alabama, Florida, Connecticut, Arkansas, Pennsylvania, Illinois, Oregon, and many more. From Bloomberg:
Basic recipes include aloe vera for moisturizing; distilleries will also add the botanicals or flavorings from their signature spirits as a twist. Portland, Ore.-based Shine Distillery & Grill isn’t treating its formula like a trade secret. “I have fielded some calls from Seattle and suggested they contact their local distilleries to tell them what we are doing,” says general manager Ryan Ruelos. “Because any distillery can do it.”
The one thing they cannot do, though, is sell their sanitizers: Sales of distilled spirits are strictly regulated by the government and could jeopardize business licenses. Instead, distilleries are giving them away to customers who come through their doors. In some cases, such as at Psychopomp Microdistillery in Bristol, England, donations from customers who take the sanitizer are being given to charity.
Around the world, alcohol is often used in toasts that relate to health: the Irish “sláinte” (health), the Mexican Spanish “salud” (to health), the Russian “vashe zdorov’ye” (to your health), the Persian “be salamati” (good health), and the Hindi “achchee sehat” (good health). These distillery-produced hand sanitizers are a toast of health from them to us, and I am very grateful for it.
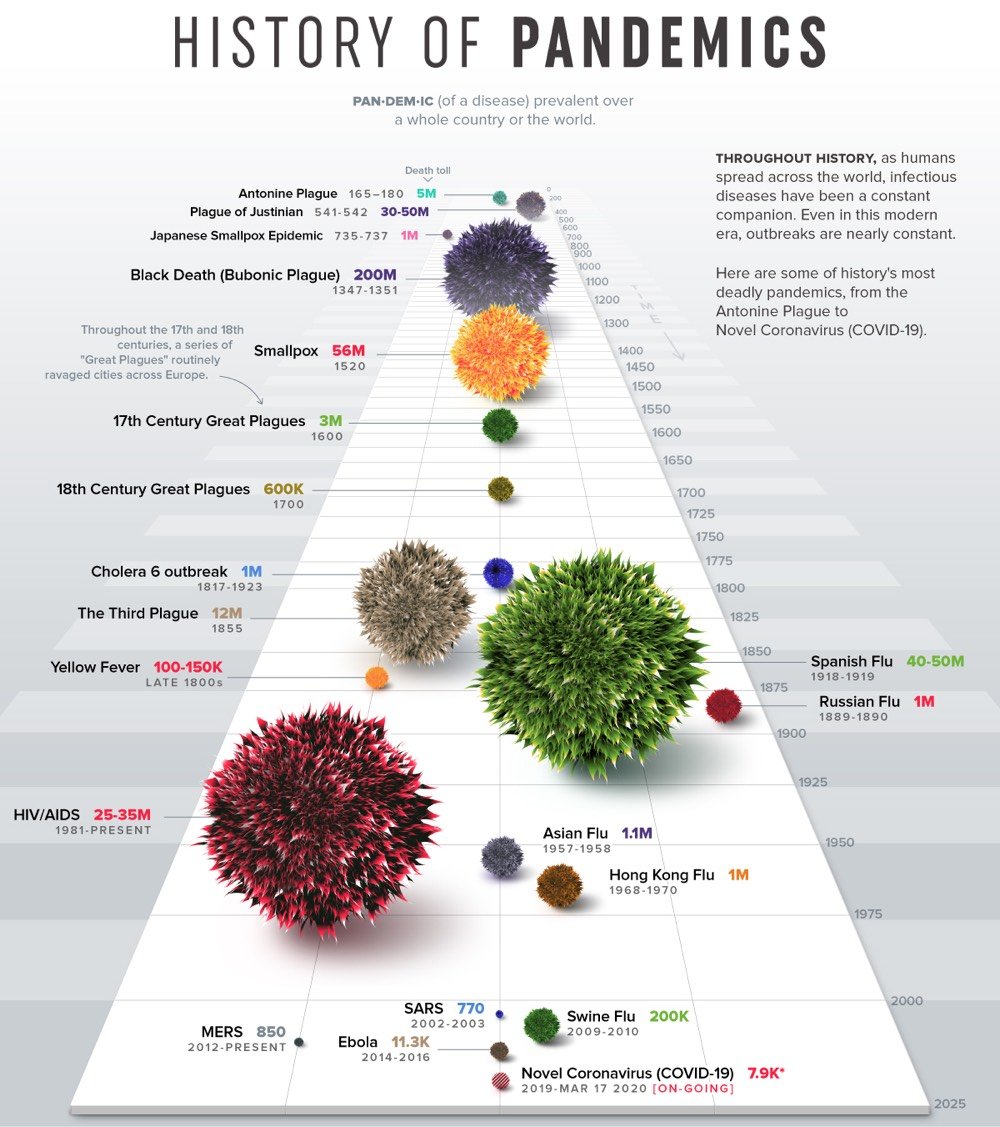
From Nicholas LePan, Visualizing the History of Pandemics.
The practice of quarantine began during the 14th century, in an effort to protect coastal cities from plague epidemics. Cautious port authorities required ships arriving in Venice from infected ports to sit at anchor for 40 days before landing — the origin of the word quarantine from the Italian “quaranta giorni”, or 40 days.
One of the first instances of relying on geography and statistical analysis was in mid-19th century London, during a cholera outbreak. In 1854, Dr. John Snow came to the conclusion that cholera was spreading via tainted water and decided to display neighborhood mortality data directly on a map. This method revealed a cluster of cases around a specific pump from which people were drawing their water from.
While the interactions created through trade and urban life play a pivotal role, it is also the virulent nature of particular diseases that indicate the trajectory of a pandemic.
One of my big takeaways from the Tracking Infectiousness section of the piece is: holy shit, look at how contagious measles is! An R0 of 16! (The common flu is about 1.5 and ebola is 2.0.) And people want to keep their children from getting vaccinated for this?!
The Washington Post made this short video that shows how Fox News personalities were talking about the COVID-19 pandemic a week or two ago — it’s a Democrat hoax!! — compared to their more recent coverage that aligns closer with the truth.
For weeks, some of Fox News’s most popular hosts downplayed the threat of the coronavirus, characterizing it as a conspiracy by media organizations and Democrats to undermine President Trump.
Fox News personalities such as Sean Hannity and Laura Ingraham accused the news media of whipping up “mass hysteria” and being “panic pushers.” Fox Business host Trish Regan called the alleged media-Democratic alliance “yet another attempt to impeach the president.”
It has never been more plain that Fox News is not journalism but conservative propaganda. They, along with Trump, some conservative members of Congress, and conservative talk radio, were just straight up lying, misleading the public, and peddling conspiracy theories until it became overwhelmingly clear that this is a serious situation, as experts had been saying for weeks. The video shows completely contradictory statements made by the same people days apart; as Andrew Kaczynski says, “what a damning indictment”. I’ll go further than that: Fox News endangered the lives of Americans with their false and misleading coverage. People will suffer and die unnecessarily because of it.
I’d urge you to show this to your red state relatives and ask them to defend Fox News as journalism, but I don’t think it will actually do any good. The whole point of propaganda is to deprive people of, as Hannah Arendt puts it, the “capacity to think and to judge”.
The moment we no longer have a free press, anything can happen. What makes it possible for a totalitarian or any other dictatorship to rule is that people are not informed; how can you have an opinion if you are not informed? If everybody always lies to you, the consequence is not that you believe the lies, but rather that nobody believes anything any longer. This is because lies, by their very nature, have to be changed, and a lying government has constantly to rewrite its own history. On the receiving end you get not only one lie-a lie which you could go on for the rest of your days-but you get a great number of lies, depending on how the political wind blows. And a people that no longer can believe anything cannot make up its mind. It is deprived not only of its capacity to act but also of its capacity to think and to judge. And with such a people you can then do what you please.

In Canada, “caremongering” groups are being organized to connect helpers with those in need during the COVID-19 pandemic.
The first “caremongering” group was set up by Mita Hans with the help of Valentina Harper and others. Valentina explained the meaning behind the name.
“Scaremongering is a big problem,” she tells the BBC. “We wanted to switch that around and get people to connect on a positive level, to connect with each other.
“It’s spread the opposite of panic in people, brought out community and camaraderie, and allowed us to tackle the needs of those who are at-risk all the time — now more than ever.”
During times of crisis, Mister Rogers urged children to “look for the helpers”. As adults, we need to step up and be those helpers, even though many of us are self-quarantined at home. (via jodi)
Free stock photo of hockey player on phone courtesy of Canada’s Internet Registration Authority.
Note: I feel the need to add a disclaimer to this post. This was a really hard thing to read for me and it might be for you too. It is a single paper from a scientific team dedicated to the study of infectious diseases — it has not been peer reviewed, the available data is changing every day (for things like death rates, transmission rates, and potential immunity), and there might be differing opinions & assumptions by other infectious disease experts that would result in a different analysis. Even so, this seems like a possibility to take seriously and I hope I’m being responsible in sharing it.
This is an excellent but extremely sobering read: Impact of non-pharmaceutical interventions (NPIs) to reduce COVID19 mortality and healthcare demand, a 20-page paper by the Imperial College COVID-19 Response Team (and a few other organizations, including the WHO Collaborating Centre for Infectious Disease Modelling).
The paper is technical in nature but mostly written in plain English so it’s pretty readable, but here is an article that summarizes the paper. It discusses the two main strategies for dealing with this epidemic (mitigation & suppression), the strengths and weaknesses of each one, and how they both may be necessary in some measure to best address the crisis. For instance, here’s a graph showing the effects of three different suppression scenarios for the US compared to critical care bed capacity:
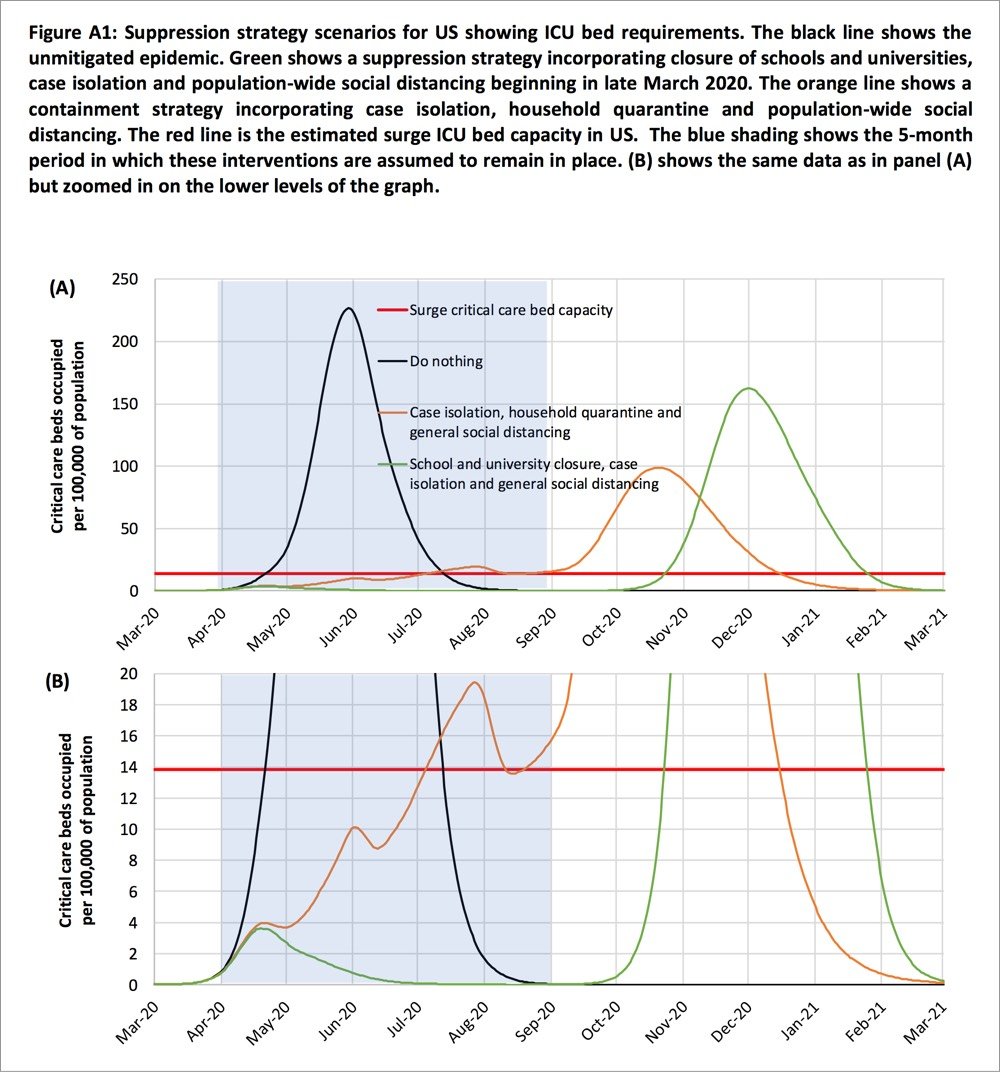
Two fundamental strategies are possible: (a) mitigation, which focuses on slowing but not necessarily stopping epidemic spread — reducing peak healthcare demand while protecting those most at risk of severe disease from infection, and (b) suppression, which aims to reverse epidemic growth, reducing case numbers to low levels and maintaining that situation indefinitely. Each policy has major challenges. We find that that optimal mitigation policies (combining home isolation of suspect cases, home quarantine of those living in the same household as suspect cases, and social distancing of the elderly and others at most risk of severe disease) might reduce peak healthcare demand by 2/3 and deaths by half. However, the resulting mitigated epidemic would still likely result in hundreds of thousands of deaths and health systems (most notably intensive care units) being overwhelmed many times over. For countries able to achieve it, this leaves suppression as the preferred policy option.
We show that in the UK and US context, suppression will minimally require a combination of social distancing of the entire population, home isolation of cases and household quarantine of their family members. This may need to be supplemented by school and university closures, though it should be recognised that such closures may have negative impacts on health systems due to increased absenteeism. The major challenge of suppression is that this type of intensive intervention package — or something equivalently effective at reducing transmission — will need to be maintained until a vaccine becomes available (potentially 18 months or more) — given that we predict that transmission will quickly rebound if interventions are relaxed. We show that intermittent social distancing — triggered by trends in disease surveillance — may allow interventions to be relaxed temporarily in relative short time windows, but measures will need to be reintroduced if or when case numbers rebound. Last, while experience in China and now South Korea show that suppression is possible in the short term, it remains to be seen whether it is possible long-term, and whether the social and economic costs of the interventions adopted thus far can be reduced.
If you missed the scale on the graph (it extends until March 2021) and the bit in there about closures, quarantine, and self-distancing measures needing to remain in place for months and months, the authors repeat that assertion throughout the paper. From the discussion section of the paper:
Overall, our results suggest that population-wide social distancing applied to the population as a whole would have the largest impact; and in combination with other interventions — notably home isolation of cases and school and university closure — has the potential to suppress transmission below the threshold of R=1 required to rapidly reduce case incidence. A minimum policy for effective suppression is therefore population-wide social distancing combined with home isolation of cases and school and university closure.
To avoid a rebound in transmission, these policies will need to be maintained until large stocks of vaccine are available to immunise the population — which could be 18 months or more. Adaptive hospital surveillance-based triggers for switching on and off population-wide social distancing and school closure offer greater robustness to uncertainty than fixed duration interventions and can be adapted for regional use (e.g. at the state level in the US). Given local epidemics are not perfectly synchronised, local policies are also more efficient and can achieve comparable levels of suppression to national policies while being in force for a slightly smaller proportion of the time. However, we estimate that for a national GB policy, social distancing would need to be in force for at least 2/3 of the time (for R0=2.4, see Table 4) until a vaccine was available.
I absolutely do not want to seem alarmist here, but if this analysis is anywhere close to being in the ballpark, it seems at least feasible that this whole thing is going to last far longer than the few weeks that people are thinking about. The concluding sentence:
However, we emphasise that is not at all certain that suppression will succeed long term; no public health intervention with such disruptive effects on society has been previously attempted for such a long duration of time. How populations and societies will respond remains unclear.
The paper is available in several languages here.
Update: Here is a short review of the Imperial College paper by Chen Shen, Nassim Nicholas Taleb, and Yaneer Bar-Yam. The important bit:
However, they make structural mistakes in analyzing outbreak response. They ignore standard Contact Tracing [2] allowing isolation of infected prior to symptoms. They also ignore door-to-door monitoring to identify cases with symptoms [3]. Their conclusions that there will be resurgent outbreaks are wrong. After a few weeks of lockdown almost all infectious people are identified and their contacts are isolated prior to symptoms and cannot infect others [4]. The outbreak can be stopped completely with no resurgence as in China, where new cases were down to one yesterday, after excluding imported international travelers that are quarantined.
If I understand this correctly, Shen et al. are saying that some tactics not taken into account by the Imperial College analysis could be hyper-effective in containing the spread of COVID-19. The big if, particularly in countries like the US and Britain that are acting like failing states is if those measures can be implemented on the scale required. (thx, ryan)
Update: The lead author of the Imperial College paper, Neil Ferguson, has likely contracted COVID-19. From his Twitter acct:
Sigh. Developed a slight dry but persistent cough yesterday and self isolated even though I felt fine. Then developed high fever at 4am today.
Ferguson says he’s still at his desk, working away.
Update: The pair of articles I linked to in this post are excellent and you should read them after reading the Imperial College paper.
Strong coronavirus measures today should only last a few weeks, there shouldn’t be a big peak of infections afterwards, and it can all be done for a reasonable cost to society, saving millions of lives along the way. If we don’t take these measures, tens of millions will be infected, many will die, along with anybody else that requires intensive care, because the healthcare system will have collapsed.
This is from a few days ago, but because the United States is a couple of weeks behind Italy in addressing the COVID-19 pandemic, what was happening there then might still be in our future if we don’t take (seemingly unreasonable but actually entirely reasonable) precautions. From Yascha Mounk’s The Extraordinary Decisions Facing Italian Doctors:
The authors, who are medical doctors, then deduce a set of concrete recommendations for how to manage these impossible choices, including this: “It may become necessary to establish an age limit for access to intensive care.”
Those who are too old to have a high likelihood of recovery, or who have too low a number of “life-years” left even if they should survive, would be left to die. This sounds cruel, but the alternative, the document argues, is no better. “In case of a total saturation of resources, maintaining the criterion of ‘first come, first served’ would amount to a decision to exclude late-arriving patients from access to intensive care.”
In addition to age, doctors and nurses are also advised to take a patient’s overall state of health into account: “The presence of comorbidities needs to be carefully evaluated.” This is in part because early studies of the virus seem to suggest that patients with serious preexisting health conditions are significantly more likely to die. But it is also because patients in a worse state of overall health could require a greater share of scarce resources to survive: “What might be a relatively short treatment course in healthier people could be longer and more resource-consuming in the case of older or more fragile patients.”
Mounk continues:
My academic training is in political and moral philosophy. I have spent countless hours in fancy seminar rooms discussing abstract moral dilemmas like the so-called trolley problem. If a train is barreling toward five innocent people who are tied to the tracks, and I could divert it by pulling the lever, but at the cost of killing an innocent bystander, should I do it?
Part of the point of all those discussions was, supposedly, to help professionals make difficult moral choices in real-world circumstances. If you are an overworked nurse battling a novel disease under the most desperate circumstances, and you simply cannot treat everyone, however hard you try, whose life should you save?
Despite those years of theory, I must admit that I have no moral judgment to make about the extraordinary document published by those brave Italian doctors. I have not the first clue whether they are recommending the right or the wrong thing.
I have been rewatching The Good Place with my kids (they love it), and all of the moral philosophy stuff underpinning the show has taken on a greater meaning over the last week or two.
Over the past week or so, echoing public health officials & epidemiologists, I’ve been trying to illustrate the often counterintuitive concept of exponential growth that you see in an epidemic and how flattening the curve can help keep people healthy and alive. But I think people have a hard time grasping what that means, personally, to them. Like, what’s one person in the face of a pandemic?
Well, epidemiologist Britta Jewell had a similar thought and came up with this brilliantly simple graph, one of the best I’ve seen in illustrating the power of exponential growth and how we as individuals can affect change:
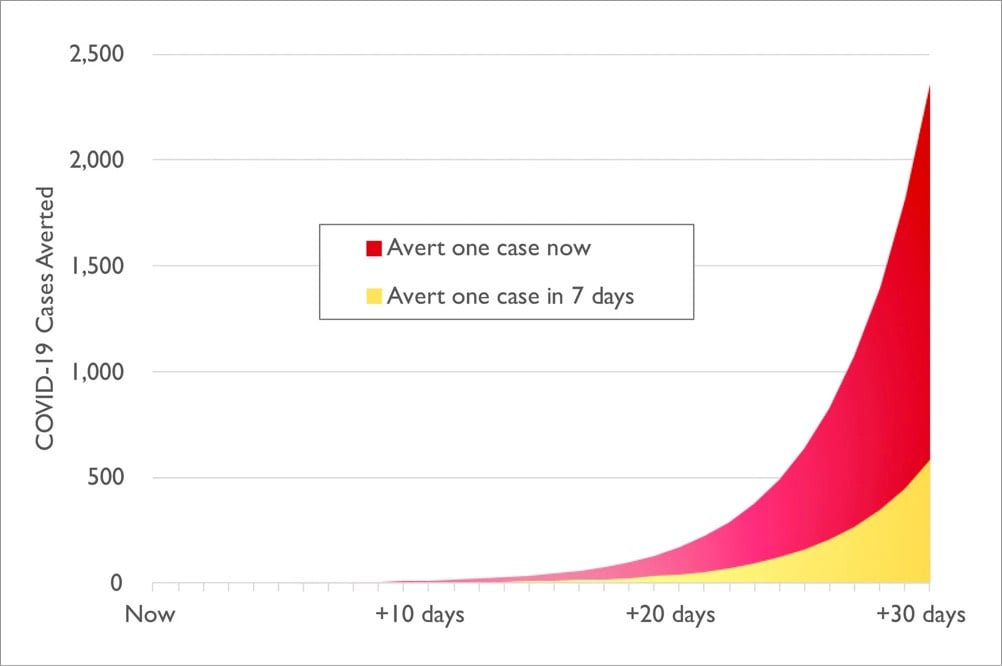
Jewell explains a bit more about what we’re looking at:
The graph illustrates the results of a thought experiment. It assumes constant 30 percent growth throughout the next month in an epidemic like the one in the U.S. right now, and compares the results of stopping one infection today — by actions such as shifting to online classes, canceling of large events and imposing travel restrictions — versus taking the same action one week from today.
The difference is stark. If you act today, you will have averted four times as many infections in the next month: roughly 2,400 averted infections, versus just 600 if you wait one week. That’s the power of averting just one infection, and obviously we would like to avert more than one.
So that’s 1800 infections averted from the actions of just one person. Assuming a somewhat conservative death rate of 1% for COVID-19, that’s 18 deaths averted. Think about that before you head out to the bar tonight or convene your book group as usual. Your actions have a lot of power in this moment; take care in how you wield it.
Coronavirus, social distancing, exponential growth, flatten the curve, pandemic, immunocompromised — those are just some of the concepts related to COVID-19 we have had to come up to speed on over the last few weeks. We should add the “paradox of preparation” to that list.
The paradox of preparation refers to how preventative measures can intuitively seem like a waste of time both before and after the fact. Most of us don’t stop brushing our teeth because the dentist didn’t find any cavities at our most recent checkup, but with larger events that have effects more difficult to gauge (like COVID-19, climate change, and Y2K), it can be hard to spur people to action. From Chris Hayes:
A doctor I spoke to today called this the “paradox of preparation” and it’s the key dynamic in all this. The only way to get ahead of the curve is to take actions that *at the time* seem like overreactions, eg: Japan closing all schools for a month with very few confirmed cases.
That was in response to Dr. James Hamblin:
The thing is if shutdowns and social distancing work perfectly and are extremely effective it will seem in retrospect like they were totally unnecessary overreactions.
Epidemiologist Mari Armstrong-Hough made a similar point earlier on Twitter:
You won’t ever know if what you did personally helped. That’s the nature of public health. When the best way to save lives is to prevent a disease rather than treat it, success often looks like an overreaction.
Preparation, prevention, regulations, and safeguards prevent catastrophes all the time, but we seldom think or hear about it because “world continues to function” is not interesting news. We have to rely on statistical analysis and the expert opinions of planners and officials in order to evaluate both crucial next steps and the effectiveness of preparatory measures after the fact, and that can be challenging for us to pay attention to. So we tend to forget that preparation & prevention is necessary and discount it the next time around.
The good news is that while unchecked epidemics grow exponentially, another thing that can also spreads exponentially is behavioral norms. The basic expert advice on how we can slow the spread of COVID-19 in our communities is pretty unambiguous — wash your hands, don’t touch your face, maintain social distance, self-quarantine, etc. — and so is the huge potential impact of those precautions on the number of people who will get infected and die. To help overcome the paradox of preparation, let’s continue to spread the word about what the experts are urging us to do. Because if we don’t, there might be a lot fewer of us around in a month or two.
Update: In the same vein, Vaughn Tan writes:
This means that any effective actions taken against coronavirus in the few days before the epidemic curve shoots upward in any country will always look unreasonable and disproportionate.
By the time those actions look reasonable and appropriate, they will be too late.
And Now Is the Time to Overreact Ian Bogost in the Atlantic:
The idea that an extreme reaction, such as closing schools and canceling events, might prove to be an overreaction that would look silly or wasteful later outweighs any other concern. It can also feel imprudent; just staying home isn’t so easy for workers who depend on weekly paychecks, and closing is a hard decision for local companies running on thin margins. But experts are saying that Americans can’t really over-prepare right now. Overreaction is good!
It’s hard to square that directive with the associations we’ve built up around overreactions. Ultimately, overreaction is a matter of knowledge-an epistemological problem. Unlike viruses or even zombies, the concept lives inside your skull rather than out in the world. The sooner we can understand how that knowledge works, and retool our action in relation to its limits, the better we’ll be able to handle the unfolding crisis.
Michael Specter writing about America’s weakened public-health system for the New Yorker:
Few people have trouble understanding the purpose of public education or public housing: they are tangible programs that, at least in theory, are designed to improve our lives. Public-health accomplishments, however, are measured in an entirely different way: success is defined by what is prevented, not by what is produced. This creates an odd psychological dynamic.
When public-health programs are successful, they are invisible, and what is invisible is almost always taken for granted. Nobody cheers when they remain untouched by a disease that they hardly knew existed. That makes it easy for shortsighted politicians to deny long-term realities. And that is what they almost always do.
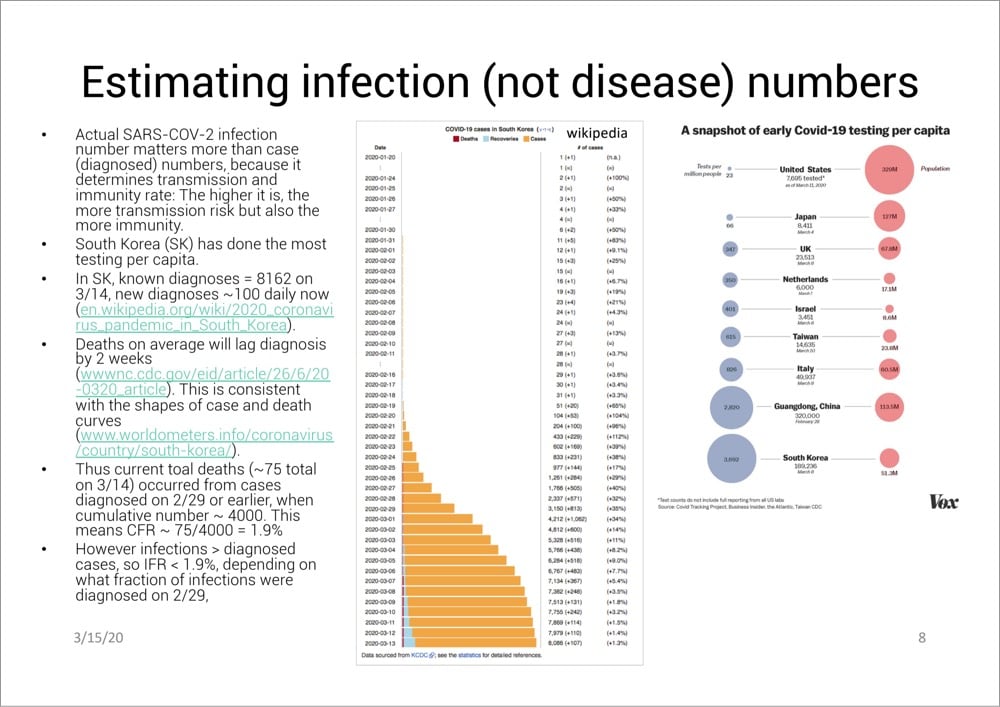
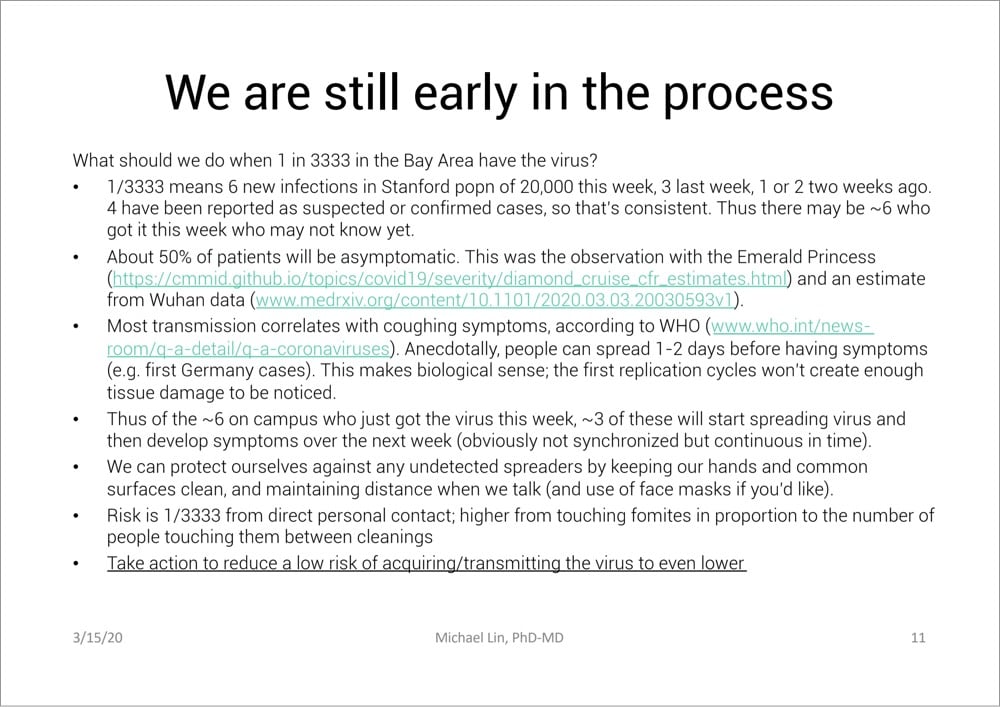
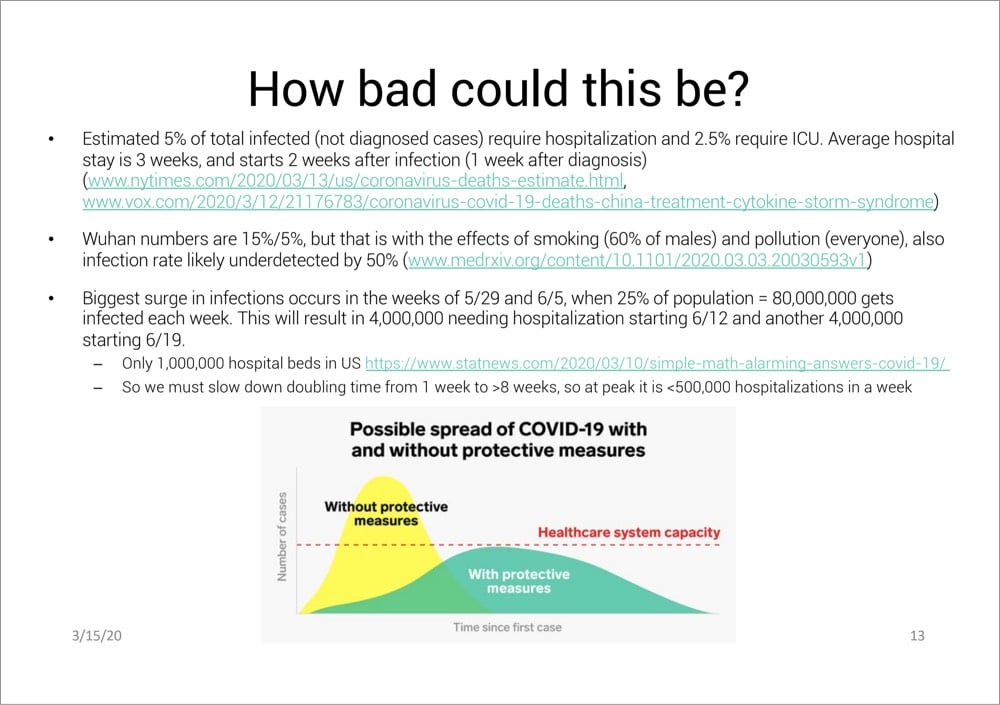
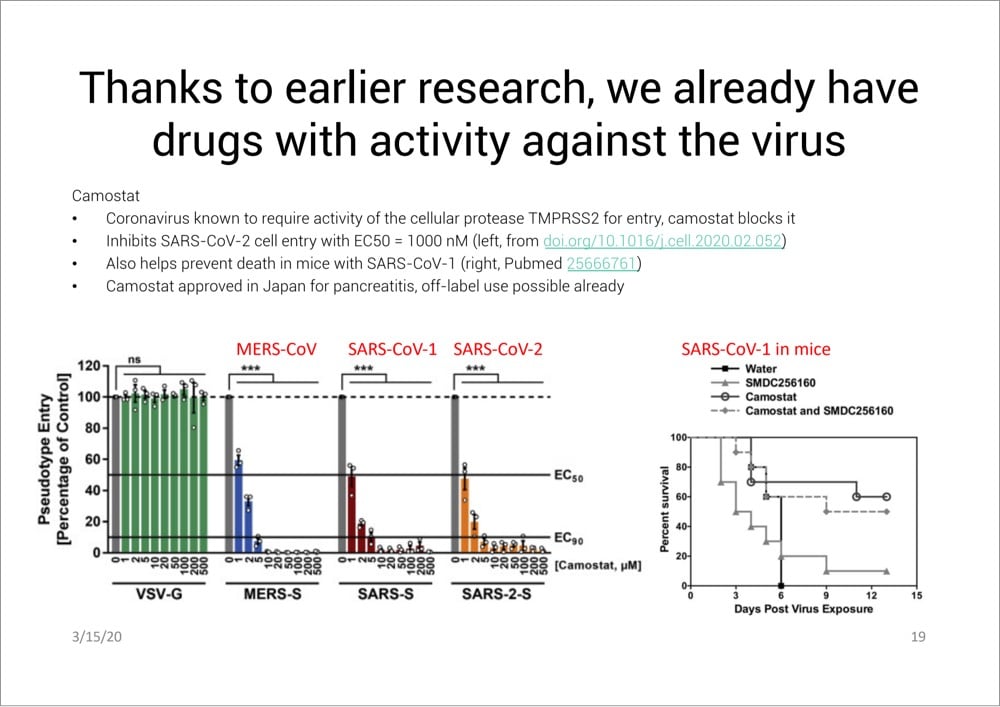
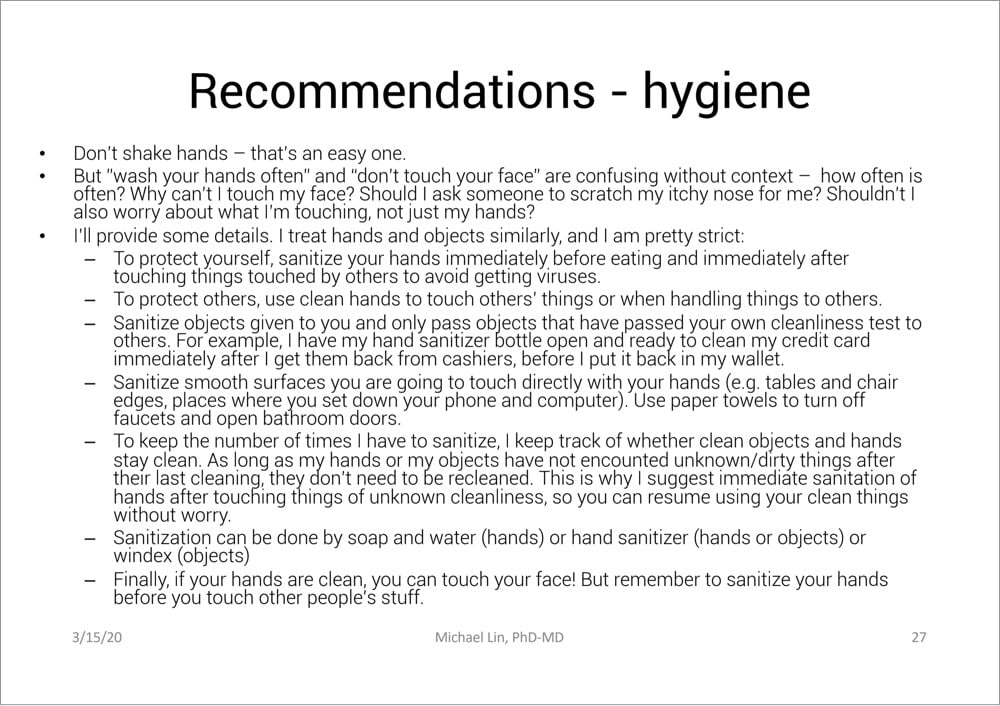
From Stanford professor of neurobiology and bioengineering Michael Lin, this is an excellent 31-page PDF presentation (Slideshare) on what we know about COVID-19 so far and how to deal with it, with extensive references to the latest research (as of 3/15). I’m going to include a few of the most interesting and important slides right here, but do read the whole thing — it is very informative.
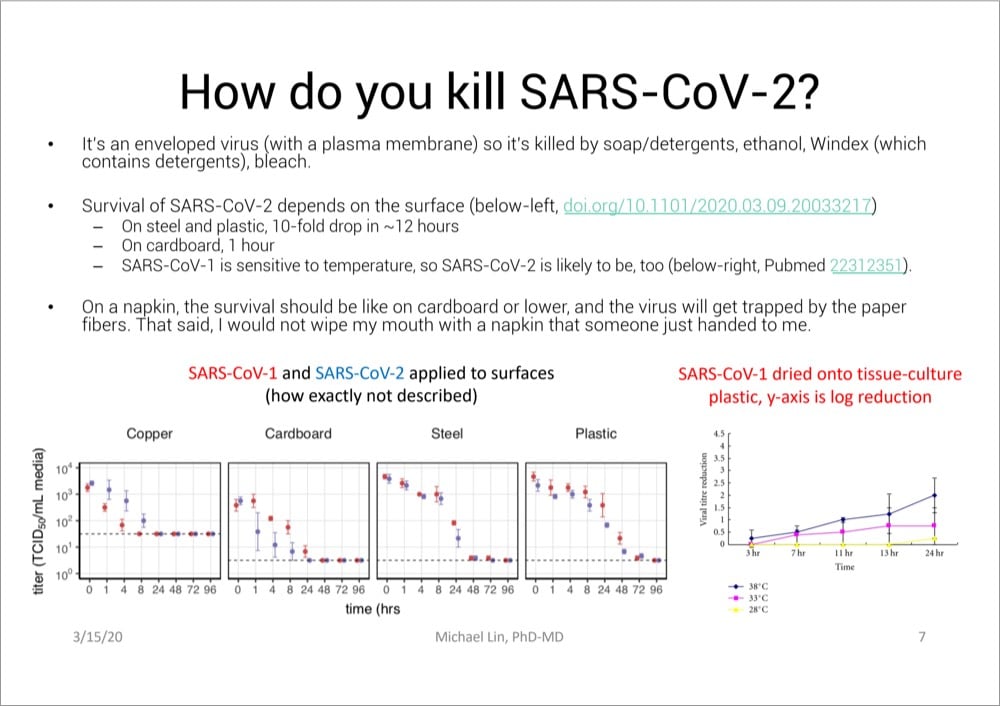
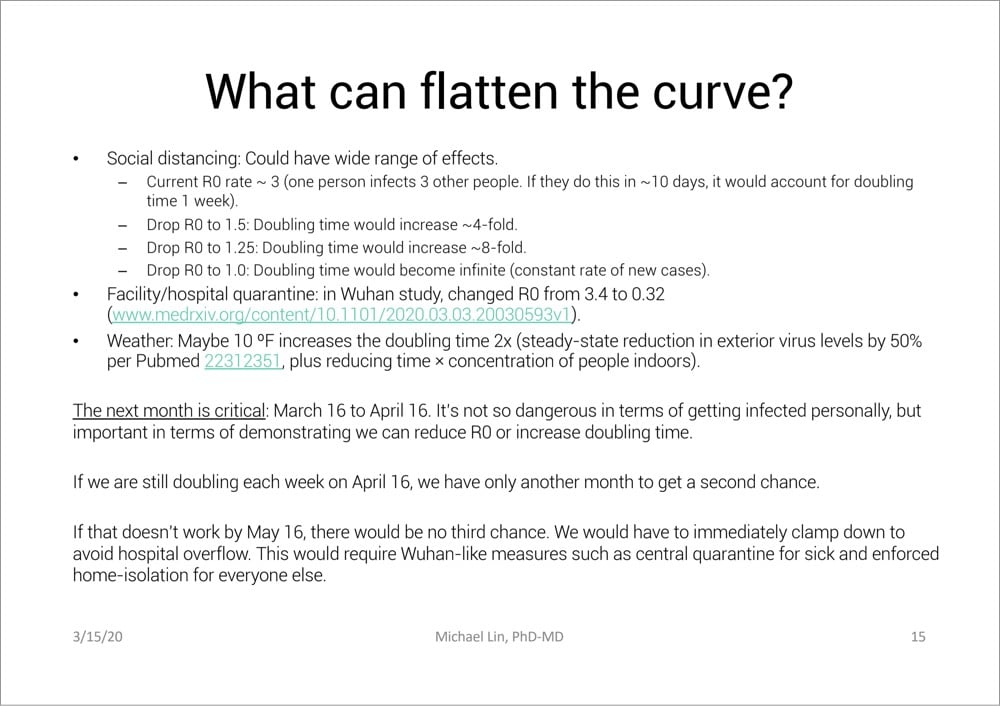
And here are a few other quotes I pulled out:
Compare to Spanish flu of 1917-1918: Cumulative infection rate 27%, IFR 2%. Spanish flu might have higher IFR than COVID-19, but medical care was much worse then (no ventilators, no drugs). In reality COVID-19 is likely the more severe disease. In any case, Spanish flu was devastating.
Large meetings that bring people from around the country are obviously a big risk. Large numbers of people who might breath the same air and touch the same things (e.g. at Biogen meeting, attendants used the same serving utensils at a buffet, and 70 got infected)
If you are young, the worry is more about transmitting virus to older people than about yourself.
Death rates will lag infection rates by 3-4 weeks (2 weeks from diagnosis but that’s 1 week from infection time on average with current testing practices)
Read Lin’s entire presentation here.
Social distancing has been recommended by epidemiologists and public health officials as a way to slow the spread of COVID-19, flatten the curve, and save lives. Avoiding rock concerts and sporting events is easy, but what about going to the grocery store or visiting with a friend? The Atlantic’s Kaitlyn Tiffany talked to a number of public health experts about The Dos and Don’ts of ‘Social Distancing’.
Q: Should I be avoiding bars and restaurants?
Cannuscio: People should avoid gathering in public places. People should be at home as much as possible. The measures that have worked to get transmission under control or at least to bend the curve, in China and South Korea, have been extreme measures to increase social distancing.
Q: Should I stop visiting elderly relatives?
Cannuscio: I think if we are fortunate enough to live near our elders and we get into the mode of seriously isolating our own families, then one person should be designated to go and visit. If we’re not in a situation where we can truly limit our own social contact, then we will be putting that elder at risk by going to visit.
In my estimation, the answers that Carolyn Cannuscio, of Penn’s Center for Public Health Initiatives, gives are the ones to follow. Dr. Asaf Bitton’s advice is even stricter:
2. No kid playdates, parties, sleepovers, or families/friends visiting each other’s houses and apartments.
This sounds extreme because it is. We are trying to create distance between family units and between individuals. It may be particularly uncomfortable for families with small children, kids with differential abilities or challenges, and for kids who simply love to play with their friends. But even if you choose only one friend to have over, you are creating new links and possibilities for the type of transmission that all of our school/work/public event closures are trying to prevent. The symptoms of coronavirus take four to five days to manifest themselves. Someone who comes over looking well can transmit the virus. Sharing food is particularly risky — I definitely do not recommend that people do so outside of their family.
They both rightly talk about how the early actions we take will end up having a big impact in limiting the damage. (Check out this video about epidemics & exponential growth if you haven’t already.) Singapore, Hong Kong, Taiwan, and other places were able to nip the epidemic in the bud in part because of aggressive social distancing practices.
People under quarantine lockdown in Italy due to the country’s COVID-19 outbreak have been singing and playing music out their windows and on their balconies to keep their spirits up while social distancing.
Here’s a Twitter thread with more videos from Salerno, Turin, Naples, Siena, Florence, etc.
No matter how much fear and panic and anxiety and negativity are on display during a crisis, it also brings out the best in people. Humans are social animals and we can’t help sharing with our neighbors, comforting one another, and coming together even when we’re physically apart.
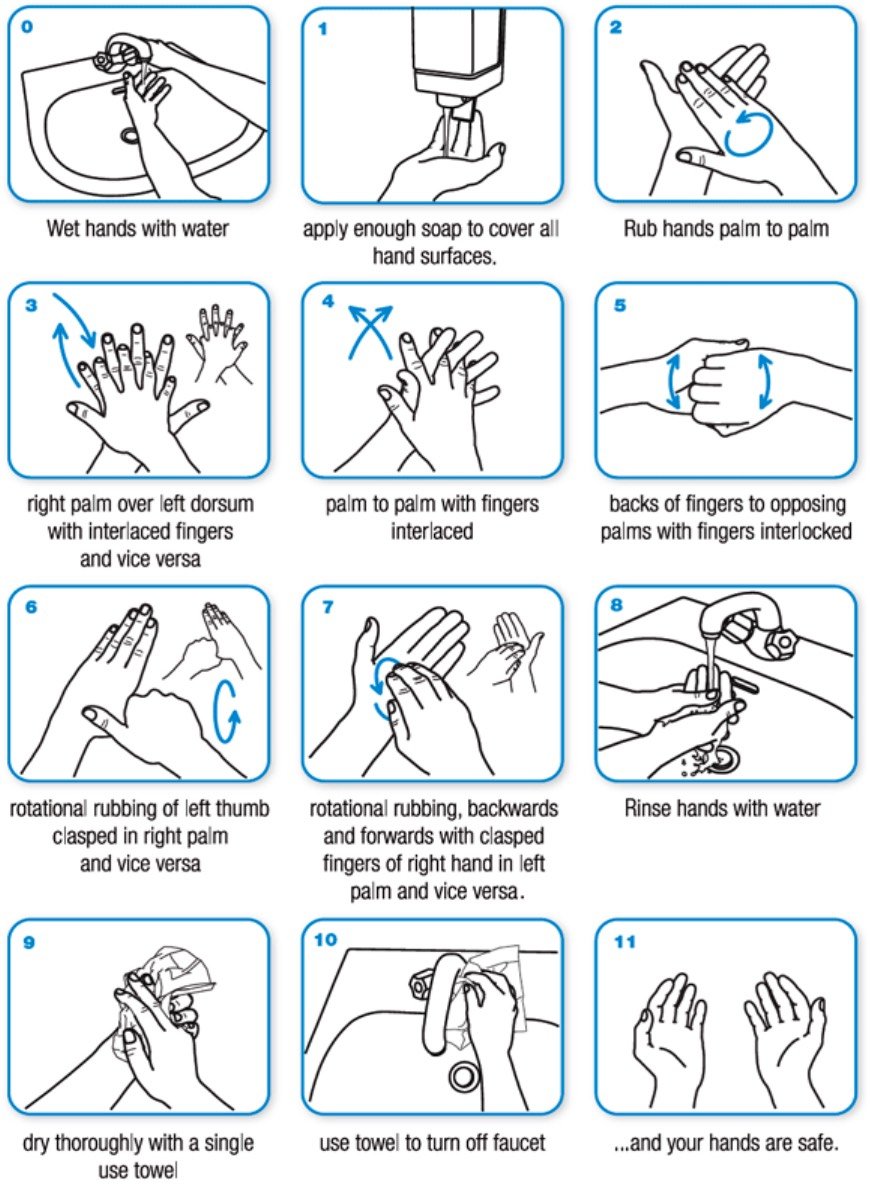
Most humans have been washing their hands since childhood, but I bet very few of us have been doing it correctly. Because of the effectiveness of hand-washing with soap in preventing the spread of COVID-19, the CDC and the WHO (and health professionals everywhere) both make it their top recommendation and provide guidance on how to do it properly: CDC hand-washing instructions, WHO hand-washing instructions.
Lather your hands by rubbing them together with the soap. Be sure to lather the backs of your hands, between your fingers, and under your nails. Scrub your hands for at least 20 seconds. Need a timer? Hum the “Happy Birthday” song from beginning to end twice.
Here’s a video from the WHO on proper hand-washing technique (and a similar one from Johns Hopkins that has subtitles):
And a graphic from the WHO:
And if you’re getting sick of singing Happy Birthday while washing your hands, a site called Wash Your Lyrics can help you make a hand-washing infographic with your favorite song’s lyrics.
According to an ongoing investigation at The Atlantic, the US has tested only about 14,000 people for COVID-19 so far (a stat CDC data seems to confirm). 14,000 out of 330 million people. Olga Khazan writes about the four main reasons why the US is so behind in testing for the virus.
Interviews with laboratory directors and public-health experts reveal a Fyre-Festival-like cascade of problems that have led to a dearth of tests at a time when America desperately needs them. The issues began with onerous requirements for the labs that make the tests, continued because of arcane hurdles that prevented researchers from getting the right supplies, and extended to a White House that seemed to lack cohesion in the pandemic’s early days. Getting out lots of tests for a new disease is a major logistical and scientific challenge, but it can be pulled off with the help of highly efficient, effective government leadership. In this case, such leadership didn’t appear to exist.
Here’s another take on the problem from a few days ago in the NY Times.
The US has bungled the situation so badly that a pair of Chinese foundations announced this morning that they were donating 500,000 testing kits and 1 million masks to the US. Last month in my Asian travelogue, I wrote that my main observation after spending three weeks in Asia was: “America is a rich country that feels like a poor country”. That we have to rely on foreign aid in situations like this is a good example of what I was referring to.
The number one recommendation on the list of protective measures for COVID-19 from both WHO and the CDC is to regularly wash your hands. The CDC in particular recommends hand-washing over using hand sanitizer.
Vox recently talked with chemistry professor Palli Thordarson about why washing with soap is so effective when dealing with coronaviruses.
The soap takes care of the virus much like it takes care of the oil in the water. “It’s almost like a crowbar; it starts to pull all the things apart,” Thordarson says.
One side of the soap molecule (the one that’s attracted to fat and repelled by water) buries its way into the virus’s fat and protein shell. Fortunately, the chemical bonds holding the virus together aren’t very strong, so this intrusion is enough to break the virus’s coat. “You pull the virus apart, you make it soluble in water, and it disintegrates,” he says.
Then the harmless shards of virus get flushed down the drain. (And even if it the soap doesn’t destroy every virus, you’ll still rid them from your hands with soap and water, as well as any grease they may be clinging to.)
And why do you need to wash for 20 seconds? Because that gives soap time to do its work.
First off, your skin is wrinkly, and it takes time for soap to penetrate into all the tiny folds and demolish the viruses that lurk within. Then the soap needs a few moments to do its chemical work. “You do need a bit of time for all the soap to interact back and forth with the virus particle,” he says. Twenty seconds should do the trick just fine.
See also Why Soap Works from the NY Times, which explains why soap & water is better than hand sanitizer in these cases:
On the whole, hand sanitizers are not as reliable as soap. Sanitizers with at least 60 percent ethanol do act similarly, defeating bacteria and viruses by destabilizing their lipid membranes. But they cannot easily remove microorganisms from the skin. There are also viruses that do not depend on lipid membranes to infect cells, as well as bacteria that protect their delicate membranes with sturdy shields of protein and sugar. Examples include bacteria that can cause meningitis, pneumonia, diarrhea and skin infections, as well as the hepatitis A virus, poliovirus, rhinoviruses and adenoviruses (frequent causes of the common cold).
Update: Thordarson also wrote an article for The Guardian on how effective soap is at killing coronavirus.
Newer posts
Older posts
Socials & More