Ten Considerations Before You Create Another Chart About COVID-19. “Visualizations are powerful for communicating information, but can also mislead, misinform, and – in the worst cases – incite panic.”
Advertise here with Carbon Ads
This site is made possible by member support. 💞
Big thanks to Arcustech for hosting the site and offering amazing tech support.
When you buy through links on kottke.org, I may earn an affiliate commission. Thanks for supporting the site!
kottke.org. home of fine hypertext products since 1998.
Beloved by 86.47% of the web.
Entries for March 2020
Some potentially positive COVID-19 news: this preprint paper suggests that SARS-CoV-2 infection confers immunity. “Our results indicated that the primary SARS-CoV-2 infection could protect from subsequent exposures.”
QuarantineChat: free service that connects random people from around the world for phone chats. “Get calls at random times and get paired with another person in a one-on-one.” It’s Chatroulette for phone calls.
“Our analyses clearly show that SARS-CoV-2 is not a laboratory construct or a purposefully manipulated virus.” It’s really great that scientists who could be working on something urgent need to spend time debunking conservative conspiracy theories.
The Coronavirus Calls for Wartime Economic Thinking. “This is not a normal economic event in any way, shape, or form. You have to be willing to think what previously would have been unthinkable.”
The perfect self-quarantine meal is @kenjilopezalt’s 3-ingredient mac & cheese. It’s as easy to make as the box kind and way more tasty. Uses shelf-stable & freezable ingredients too.
Caremongering

In Canada, “caremongering” groups are being organized to connect helpers with those in need during the COVID-19 pandemic.
The first “caremongering” group was set up by Mita Hans with the help of Valentina Harper and others. Valentina explained the meaning behind the name.
“Scaremongering is a big problem,” she tells the BBC. “We wanted to switch that around and get people to connect on a positive level, to connect with each other.
“It’s spread the opposite of panic in people, brought out community and camaraderie, and allowed us to tackle the needs of those who are at-risk all the time — now more than ever.”
During times of crisis, Mister Rogers urged children to “look for the helpers”. As adults, we need to step up and be those helpers, even though many of us are self-quarantined at home. (via jodi)
Free stock photo of hockey player on phone courtesy of Canada’s Internet Registration Authority.
We May Be In This for the Long Haul…
Note: I feel the need to add a disclaimer to this post. This was a really hard thing to read for me and it might be for you too. It is a single paper from a scientific team dedicated to the study of infectious diseases — it has not been peer reviewed, the available data is changing every day (for things like death rates, transmission rates, and potential immunity), and there might be differing opinions & assumptions by other infectious disease experts that would result in a different analysis. Even so, this seems like a possibility to take seriously and I hope I’m being responsible in sharing it.
This is an excellent but extremely sobering read: Impact of non-pharmaceutical interventions (NPIs) to reduce COVID19 mortality and healthcare demand, a 20-page paper by the Imperial College COVID-19 Response Team (and a few other organizations, including the WHO Collaborating Centre for Infectious Disease Modelling).
The paper is technical in nature but mostly written in plain English so it’s pretty readable, but here is an article that summarizes the paper. It discusses the two main strategies for dealing with this epidemic (mitigation & suppression), the strengths and weaknesses of each one, and how they both may be necessary in some measure to best address the crisis. For instance, here’s a graph showing the effects of three different suppression scenarios for the US compared to critical care bed capacity:
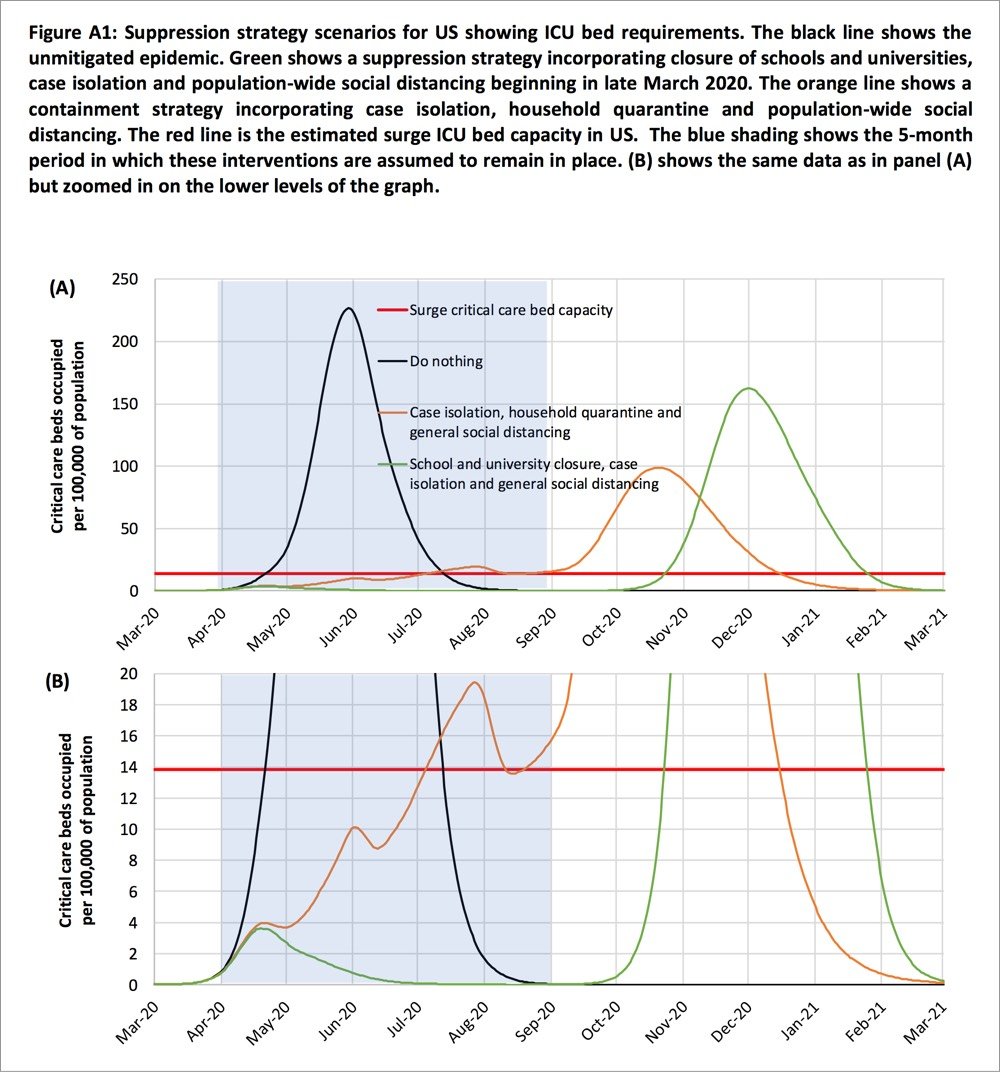
Two fundamental strategies are possible: (a) mitigation, which focuses on slowing but not necessarily stopping epidemic spread — reducing peak healthcare demand while protecting those most at risk of severe disease from infection, and (b) suppression, which aims to reverse epidemic growth, reducing case numbers to low levels and maintaining that situation indefinitely. Each policy has major challenges. We find that that optimal mitigation policies (combining home isolation of suspect cases, home quarantine of those living in the same household as suspect cases, and social distancing of the elderly and others at most risk of severe disease) might reduce peak healthcare demand by 2/3 and deaths by half. However, the resulting mitigated epidemic would still likely result in hundreds of thousands of deaths and health systems (most notably intensive care units) being overwhelmed many times over. For countries able to achieve it, this leaves suppression as the preferred policy option.
We show that in the UK and US context, suppression will minimally require a combination of social distancing of the entire population, home isolation of cases and household quarantine of their family members. This may need to be supplemented by school and university closures, though it should be recognised that such closures may have negative impacts on health systems due to increased absenteeism. The major challenge of suppression is that this type of intensive intervention package — or something equivalently effective at reducing transmission — will need to be maintained until a vaccine becomes available (potentially 18 months or more) — given that we predict that transmission will quickly rebound if interventions are relaxed. We show that intermittent social distancing — triggered by trends in disease surveillance — may allow interventions to be relaxed temporarily in relative short time windows, but measures will need to be reintroduced if or when case numbers rebound. Last, while experience in China and now South Korea show that suppression is possible in the short term, it remains to be seen whether it is possible long-term, and whether the social and economic costs of the interventions adopted thus far can be reduced.
If you missed the scale on the graph (it extends until March 2021) and the bit in there about closures, quarantine, and self-distancing measures needing to remain in place for months and months, the authors repeat that assertion throughout the paper. From the discussion section of the paper:
Overall, our results suggest that population-wide social distancing applied to the population as a whole would have the largest impact; and in combination with other interventions — notably home isolation of cases and school and university closure — has the potential to suppress transmission below the threshold of R=1 required to rapidly reduce case incidence. A minimum policy for effective suppression is therefore population-wide social distancing combined with home isolation of cases and school and university closure.
To avoid a rebound in transmission, these policies will need to be maintained until large stocks of vaccine are available to immunise the population — which could be 18 months or more. Adaptive hospital surveillance-based triggers for switching on and off population-wide social distancing and school closure offer greater robustness to uncertainty than fixed duration interventions and can be adapted for regional use (e.g. at the state level in the US). Given local epidemics are not perfectly synchronised, local policies are also more efficient and can achieve comparable levels of suppression to national policies while being in force for a slightly smaller proportion of the time. However, we estimate that for a national GB policy, social distancing would need to be in force for at least 2/3 of the time (for R0=2.4, see Table 4) until a vaccine was available.
I absolutely do not want to seem alarmist here, but if this analysis is anywhere close to being in the ballpark, it seems at least feasible that this whole thing is going to last far longer than the few weeks that people are thinking about. The concluding sentence:
However, we emphasise that is not at all certain that suppression will succeed long term; no public health intervention with such disruptive effects on society has been previously attempted for such a long duration of time. How populations and societies will respond remains unclear.
The paper is available in several languages here.
Update: Here is a short review of the Imperial College paper by Chen Shen, Nassim Nicholas Taleb, and Yaneer Bar-Yam. The important bit:
However, they make structural mistakes in analyzing outbreak response. They ignore standard Contact Tracing [2] allowing isolation of infected prior to symptoms. They also ignore door-to-door monitoring to identify cases with symptoms [3]. Their conclusions that there will be resurgent outbreaks are wrong. After a few weeks of lockdown almost all infectious people are identified and their contacts are isolated prior to symptoms and cannot infect others [4]. The outbreak can be stopped completely with no resurgence as in China, where new cases were down to one yesterday, after excluding imported international travelers that are quarantined.
If I understand this correctly, Shen et al. are saying that some tactics not taken into account by the Imperial College analysis could be hyper-effective in containing the spread of COVID-19. The big if, particularly in countries like the US and Britain that are acting like failing states is if those measures can be implemented on the scale required. (thx, ryan)
Update: The lead author of the Imperial College paper, Neil Ferguson, has likely contracted COVID-19. From his Twitter acct:
Sigh. Developed a slight dry but persistent cough yesterday and self isolated even though I felt fine. Then developed high fever at 4am today.
Ferguson says he’s still at his desk, working away.
Update: The pair of articles I linked to in this post are excellent and you should read them after reading the Imperial College paper.
Strong coronavirus measures today should only last a few weeks, there shouldn’t be a big peak of infections afterwards, and it can all be done for a reasonable cost to society, saving millions of lives along the way. If we don’t take these measures, tens of millions will be infected, many will die, along with anybody else that requires intensive care, because the healthcare system will have collapsed.
Moral Choices in an Overwhelming Emergency
This is from a few days ago, but because the United States is a couple of weeks behind Italy in addressing the COVID-19 pandemic, what was happening there then might still be in our future if we don’t take (seemingly unreasonable but actually entirely reasonable) precautions. From Yascha Mounk’s The Extraordinary Decisions Facing Italian Doctors:
The authors, who are medical doctors, then deduce a set of concrete recommendations for how to manage these impossible choices, including this: “It may become necessary to establish an age limit for access to intensive care.”
Those who are too old to have a high likelihood of recovery, or who have too low a number of “life-years” left even if they should survive, would be left to die. This sounds cruel, but the alternative, the document argues, is no better. “In case of a total saturation of resources, maintaining the criterion of ‘first come, first served’ would amount to a decision to exclude late-arriving patients from access to intensive care.”
In addition to age, doctors and nurses are also advised to take a patient’s overall state of health into account: “The presence of comorbidities needs to be carefully evaluated.” This is in part because early studies of the virus seem to suggest that patients with serious preexisting health conditions are significantly more likely to die. But it is also because patients in a worse state of overall health could require a greater share of scarce resources to survive: “What might be a relatively short treatment course in healthier people could be longer and more resource-consuming in the case of older or more fragile patients.”
Mounk continues:
My academic training is in political and moral philosophy. I have spent countless hours in fancy seminar rooms discussing abstract moral dilemmas like the so-called trolley problem. If a train is barreling toward five innocent people who are tied to the tracks, and I could divert it by pulling the lever, but at the cost of killing an innocent bystander, should I do it?
Part of the point of all those discussions was, supposedly, to help professionals make difficult moral choices in real-world circumstances. If you are an overworked nurse battling a novel disease under the most desperate circumstances, and you simply cannot treat everyone, however hard you try, whose life should you save?
Despite those years of theory, I must admit that I have no moral judgment to make about the extraordinary document published by those brave Italian doctors. I have not the first clue whether they are recommending the right or the wrong thing.
I have been rewatching The Good Place with my kids (they love it), and all of the moral philosophy stuff underpinning the show has taken on a greater meaning over the last week or two.
The airlines may want a federal bailout, but after making billions of dollars over the past decade, perhaps they do not deserve it. “Before providing them any assistance, we must demand that they change how they treat their customers and employees.”
The Power of the Individual in an Exponential Crisis
Over the past week or so, echoing public health officials & epidemiologists, I’ve been trying to illustrate the often counterintuitive concept of exponential growth that you see in an epidemic and how flattening the curve can help keep people healthy and alive. But I think people have a hard time grasping what that means, personally, to them. Like, what’s one person in the face of a pandemic?
Well, epidemiologist Britta Jewell had a similar thought and came up with this brilliantly simple graph, one of the best I’ve seen in illustrating the power of exponential growth and how we as individuals can affect change:
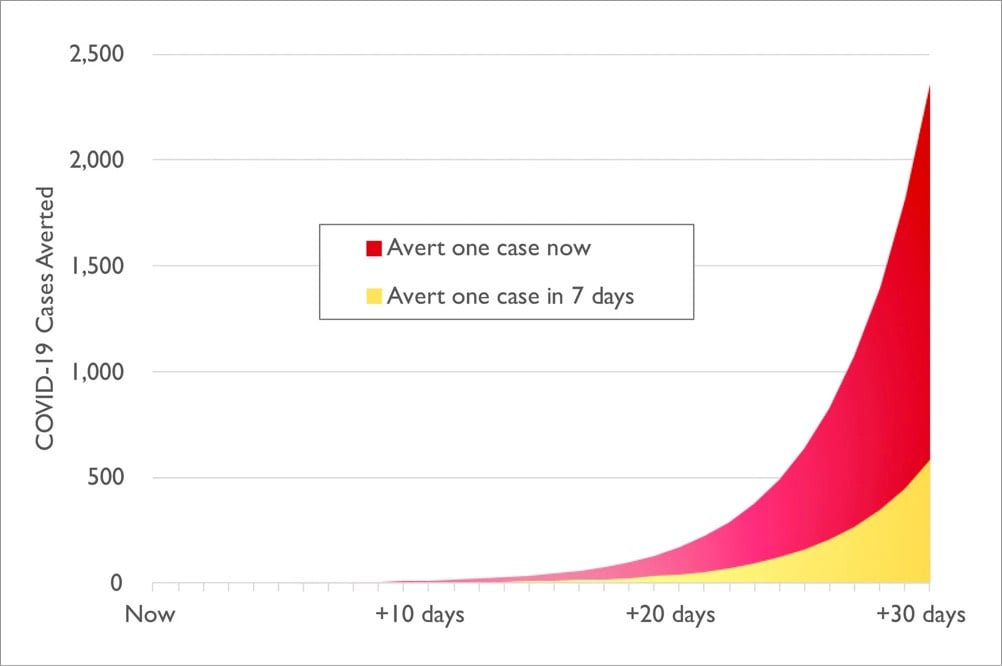
Jewell explains a bit more about what we’re looking at:
The graph illustrates the results of a thought experiment. It assumes constant 30 percent growth throughout the next month in an epidemic like the one in the U.S. right now, and compares the results of stopping one infection today — by actions such as shifting to online classes, canceling of large events and imposing travel restrictions — versus taking the same action one week from today.
The difference is stark. If you act today, you will have averted four times as many infections in the next month: roughly 2,400 averted infections, versus just 600 if you wait one week. That’s the power of averting just one infection, and obviously we would like to avert more than one.
So that’s 1800 infections averted from the actions of just one person. Assuming a somewhat conservative death rate of 1% for COVID-19, that’s 18 deaths averted. Think about that before you head out to the bar tonight or convene your book group as usual. Your actions have a lot of power in this moment; take care in how you wield it.
Canada just announced it has closed its borders to anyone who isn’t a citizen or permanent resident. US citizens are exempt (for now).
Working and Learning from Home with Young Children, good advice on how to work from home and homeschool at the same time from Erin Kissane. “Don’t be Captain Homeschool on day one.”
The Paradox of Preparation
Coronavirus, social distancing, exponential growth, flatten the curve, pandemic, immunocompromised — those are just some of the concepts related to COVID-19 we have had to come up to speed on over the last few weeks. We should add the “paradox of preparation” to that list.
The paradox of preparation refers to how preventative measures can intuitively seem like a waste of time both before and after the fact. Most of us don’t stop brushing our teeth because the dentist didn’t find any cavities at our most recent checkup, but with larger events that have effects more difficult to gauge (like COVID-19, climate change, and Y2K), it can be hard to spur people to action. From Chris Hayes:
A doctor I spoke to today called this the “paradox of preparation” and it’s the key dynamic in all this. The only way to get ahead of the curve is to take actions that *at the time* seem like overreactions, eg: Japan closing all schools for a month with very few confirmed cases.
That was in response to Dr. James Hamblin:
The thing is if shutdowns and social distancing work perfectly and are extremely effective it will seem in retrospect like they were totally unnecessary overreactions.
Epidemiologist Mari Armstrong-Hough made a similar point earlier on Twitter:
You won’t ever know if what you did personally helped. That’s the nature of public health. When the best way to save lives is to prevent a disease rather than treat it, success often looks like an overreaction.
Preparation, prevention, regulations, and safeguards prevent catastrophes all the time, but we seldom think or hear about it because “world continues to function” is not interesting news. We have to rely on statistical analysis and the expert opinions of planners and officials in order to evaluate both crucial next steps and the effectiveness of preparatory measures after the fact, and that can be challenging for us to pay attention to. So we tend to forget that preparation & prevention is necessary and discount it the next time around.
The good news is that while unchecked epidemics grow exponentially, another thing that can also spreads exponentially is behavioral norms. The basic expert advice on how we can slow the spread of COVID-19 in our communities is pretty unambiguous — wash your hands, don’t touch your face, maintain social distance, self-quarantine, etc. — and so is the huge potential impact of those precautions on the number of people who will get infected and die. To help overcome the paradox of preparation, let’s continue to spread the word about what the experts are urging us to do. Because if we don’t, there might be a lot fewer of us around in a month or two.
Update: In the same vein, Vaughn Tan writes:
This means that any effective actions taken against coronavirus in the few days before the epidemic curve shoots upward in any country will always look unreasonable and disproportionate.
By the time those actions look reasonable and appropriate, they will be too late.
And Now Is the Time to Overreact Ian Bogost in the Atlantic:
The idea that an extreme reaction, such as closing schools and canceling events, might prove to be an overreaction that would look silly or wasteful later outweighs any other concern. It can also feel imprudent; just staying home isn’t so easy for workers who depend on weekly paychecks, and closing is a hard decision for local companies running on thin margins. But experts are saying that Americans can’t really over-prepare right now. Overreaction is good!
It’s hard to square that directive with the associations we’ve built up around overreactions. Ultimately, overreaction is a matter of knowledge-an epistemological problem. Unlike viruses or even zombies, the concept lives inside your skull rather than out in the world. The sooner we can understand how that knowledge works, and retool our action in relation to its limits, the better we’ll be able to handle the unfolding crisis.
Michael Specter writing about America’s weakened public-health system for the New Yorker:
Few people have trouble understanding the purpose of public education or public housing: they are tangible programs that, at least in theory, are designed to improve our lives. Public-health accomplishments, however, are measured in an entirely different way: success is defined by what is prevented, not by what is produced. This creates an odd psychological dynamic.
When public-health programs are successful, they are invisible, and what is invisible is almost always taken for granted. Nobody cheers when they remain untouched by a disease that they hardly knew existed. That makes it easy for shortsighted politicians to deny long-term realities. And that is what they almost always do.
Interactive chart where you can toggle between “weak quarantine like Italy” and “strong quarantine like South Korea” for your locale. If Massachusetts acts like Italy, there will be “widespread ventilator shortages” by Mar 25.
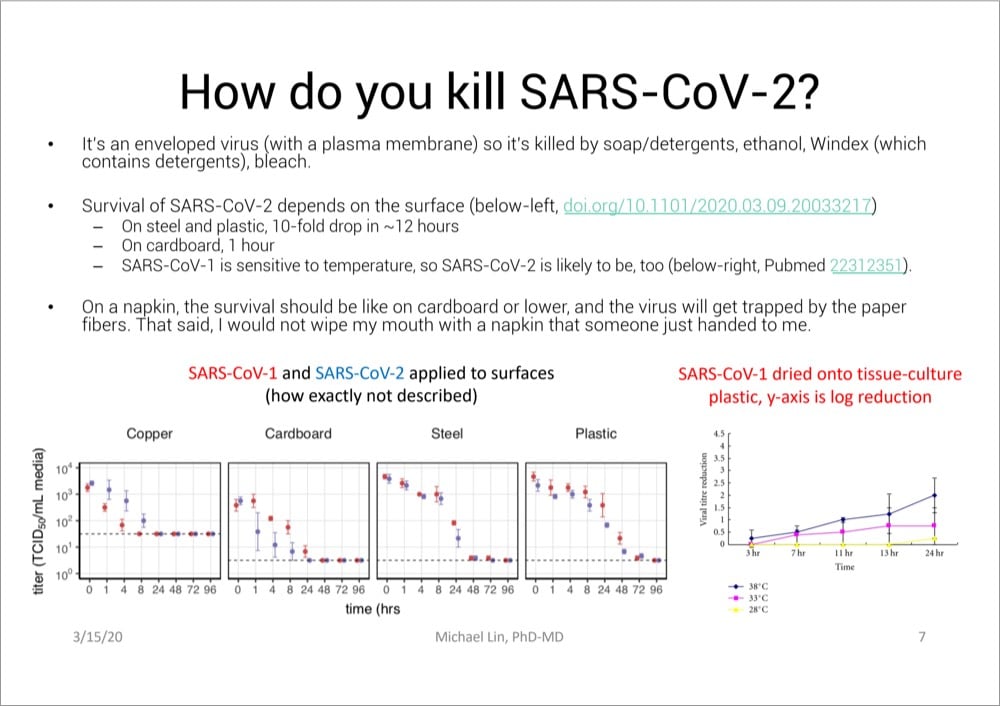
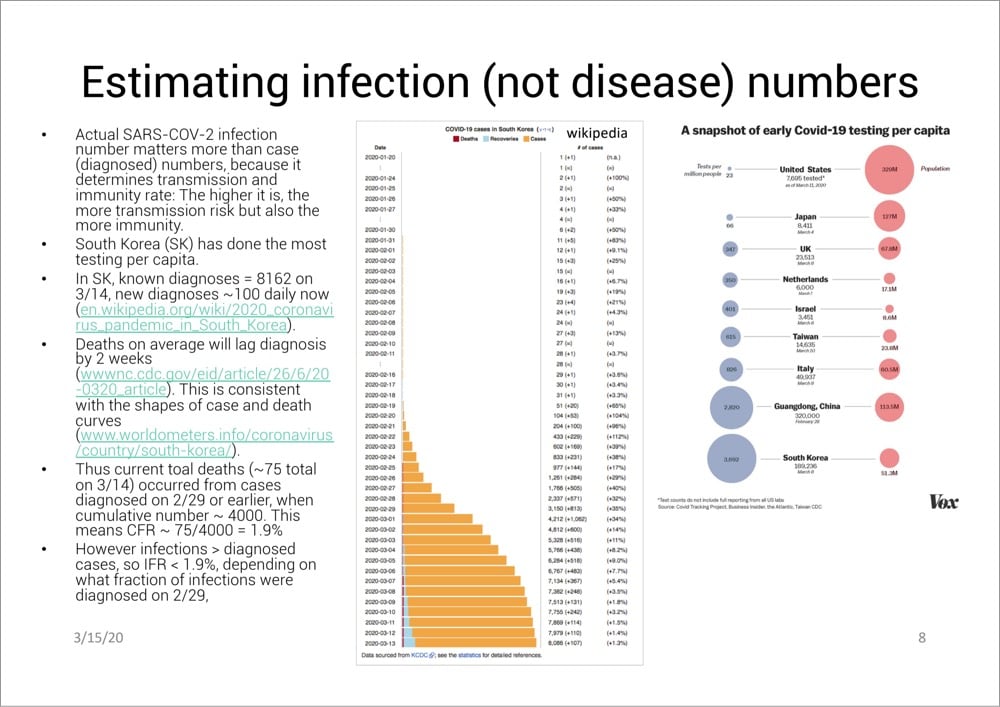
Excellent Presentation on the Latest COVID-19 Research, Hygiene Tips, and Treatment Options
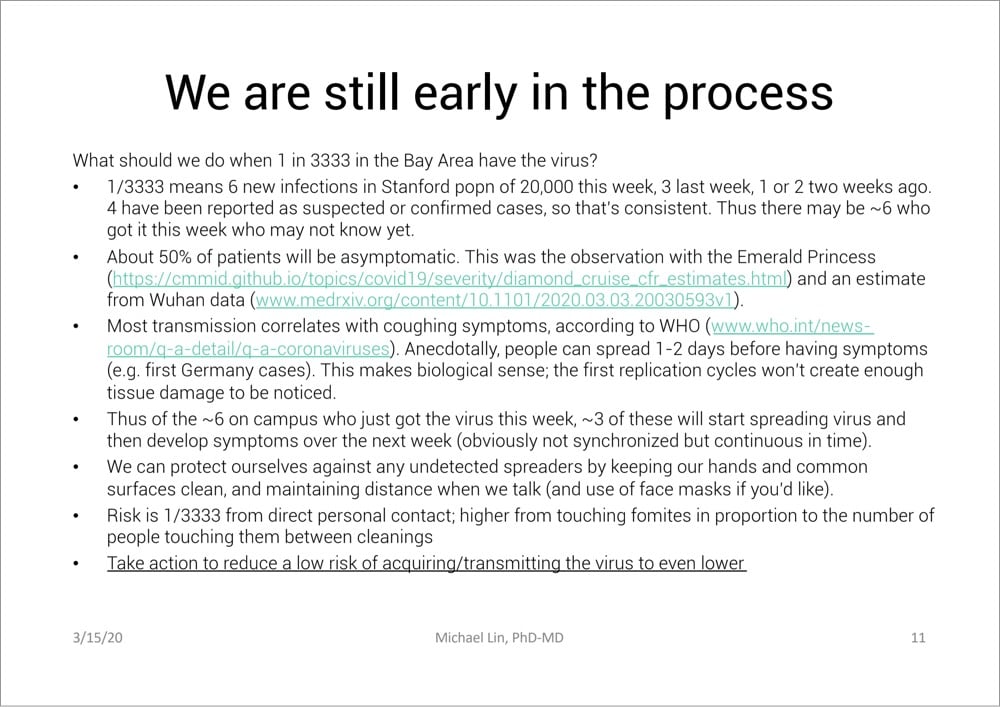
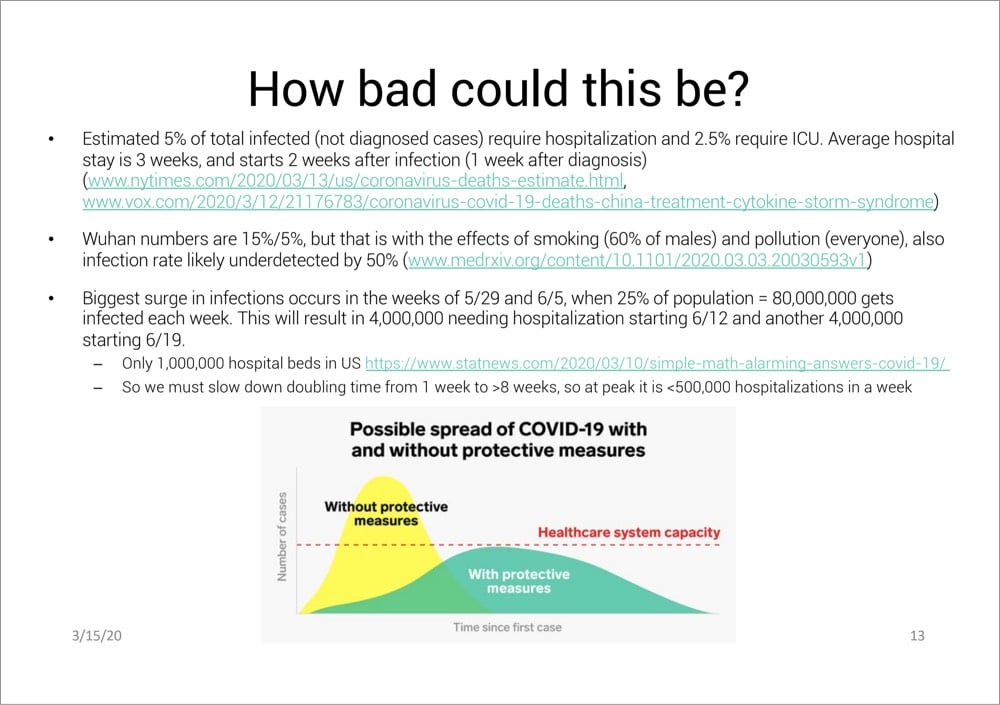
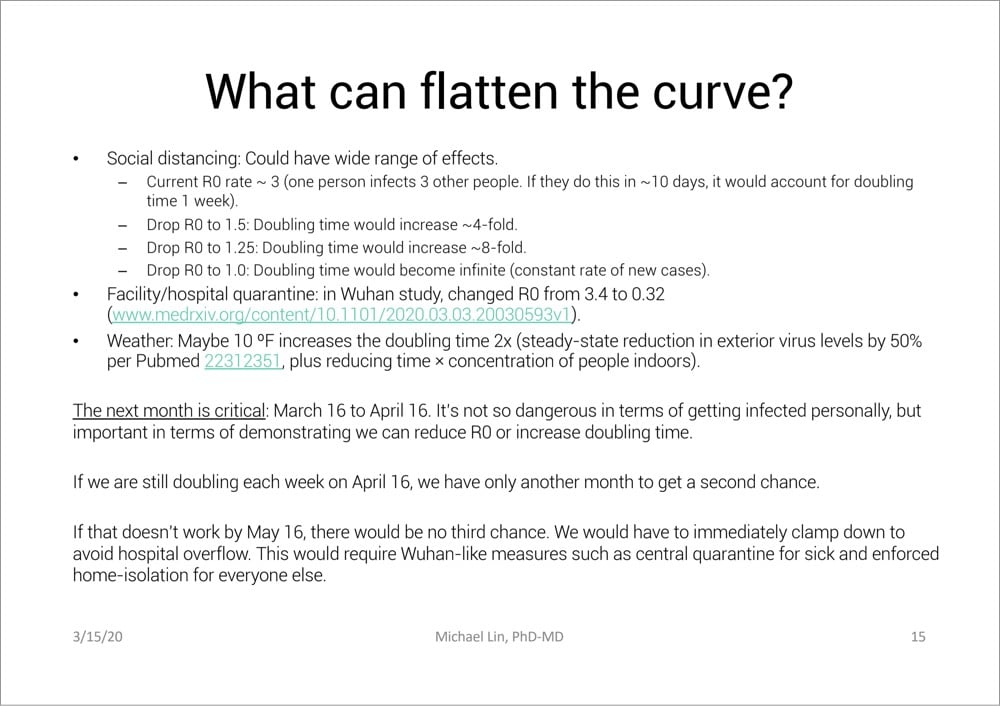
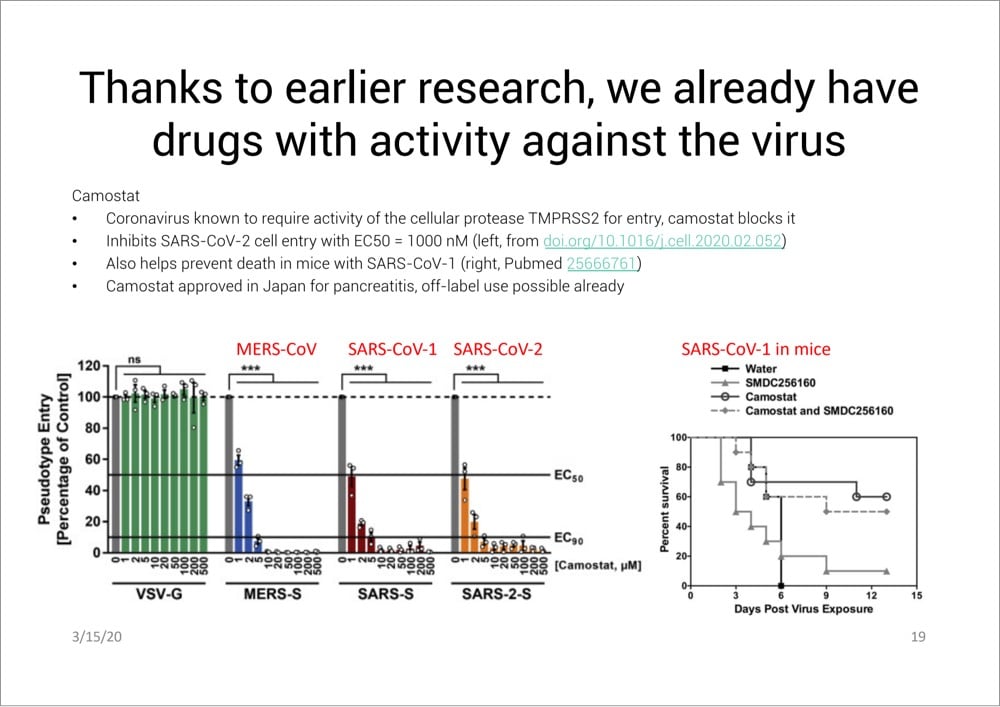
From Stanford professor of neurobiology and bioengineering Michael Lin, this is an excellent 31-page PDF presentation (Slideshare) on what we know about COVID-19 so far and how to deal with it, with extensive references to the latest research (as of 3/15). I’m going to include a few of the most interesting and important slides right here, but do read the whole thing — it is very informative.
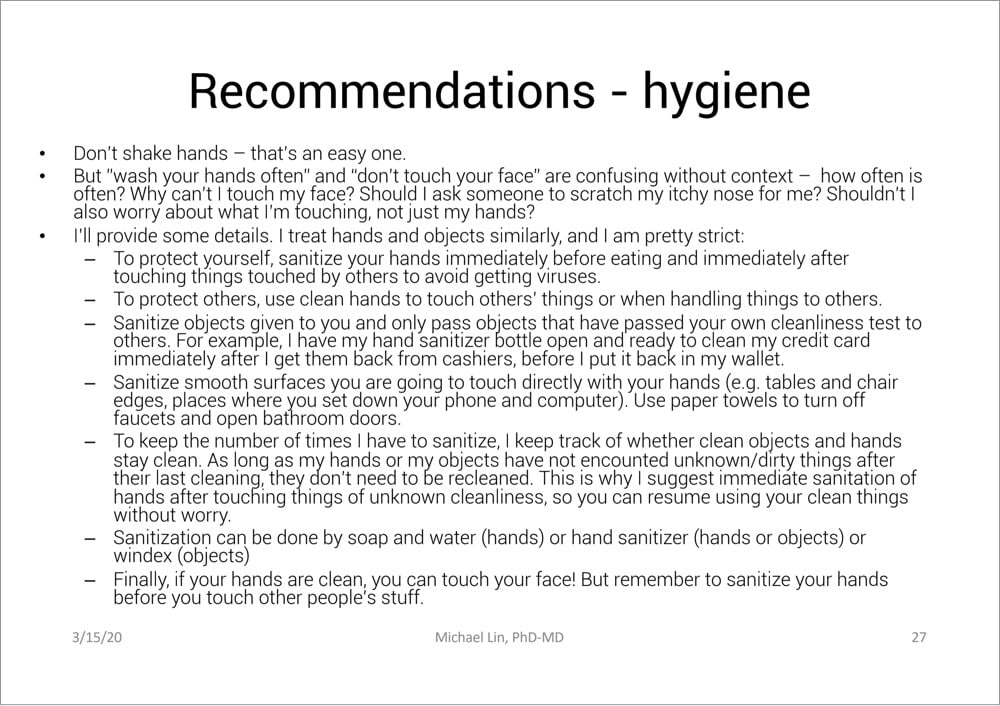
And here are a few other quotes I pulled out:
Compare to Spanish flu of 1917-1918: Cumulative infection rate 27%, IFR 2%. Spanish flu might have higher IFR than COVID-19, but medical care was much worse then (no ventilators, no drugs). In reality COVID-19 is likely the more severe disease. In any case, Spanish flu was devastating.
Large meetings that bring people from around the country are obviously a big risk. Large numbers of people who might breath the same air and touch the same things (e.g. at Biogen meeting, attendants used the same serving utensils at a buffet, and 70 got infected)
If you are young, the worry is more about transmitting virus to older people than about yourself.
Death rates will lag infection rates by 3-4 weeks (2 weeks from diagnosis but that’s 1 week from infection time on average with current testing practices)
Read Lin’s entire presentation here.
NYC schools are closing tomorrow to help slow spread of the COVID-19 pandemic. They will remain closed through at least April 20.
A simple COVID-19 simulator. You can really see how early efforts (like social distancing) can result in huge changes in infections & deaths down the road. Like tens of millions vs thousands.
This is an excellent simulation of how COVID-19 could play out under 4 different scenarios: a) do nothing, b) attempted quarantine, c) moderate social distancing, d) extreme social distancing. The differences are stark!
Expert Advice and Harsh Truths About Social Distancing
Social distancing has been recommended by epidemiologists and public health officials as a way to slow the spread of COVID-19, flatten the curve, and save lives. Avoiding rock concerts and sporting events is easy, but what about going to the grocery store or visiting with a friend? The Atlantic’s Kaitlyn Tiffany talked to a number of public health experts about The Dos and Don’ts of ‘Social Distancing’.
Q: Should I be avoiding bars and restaurants?
Cannuscio: People should avoid gathering in public places. People should be at home as much as possible. The measures that have worked to get transmission under control or at least to bend the curve, in China and South Korea, have been extreme measures to increase social distancing.
Q: Should I stop visiting elderly relatives?
Cannuscio: I think if we are fortunate enough to live near our elders and we get into the mode of seriously isolating our own families, then one person should be designated to go and visit. If we’re not in a situation where we can truly limit our own social contact, then we will be putting that elder at risk by going to visit.
In my estimation, the answers that Carolyn Cannuscio, of Penn’s Center for Public Health Initiatives, gives are the ones to follow. Dr. Asaf Bitton’s advice is even stricter:
2. No kid playdates, parties, sleepovers, or families/friends visiting each other’s houses and apartments.
This sounds extreme because it is. We are trying to create distance between family units and between individuals. It may be particularly uncomfortable for families with small children, kids with differential abilities or challenges, and for kids who simply love to play with their friends. But even if you choose only one friend to have over, you are creating new links and possibilities for the type of transmission that all of our school/work/public event closures are trying to prevent. The symptoms of coronavirus take four to five days to manifest themselves. Someone who comes over looking well can transmit the virus. Sharing food is particularly risky — I definitely do not recommend that people do so outside of their family.
They both rightly talk about how the early actions we take will end up having a big impact in limiting the damage. (Check out this video about epidemics & exponential growth if you haven’t already.) Singapore, Hong Kong, Taiwan, and other places were able to nip the epidemic in the bud in part because of aggressive social distancing practices.
The number of obituaries listed in the local newspaper in Bergamo, Italy has skyrocketed. Feb 9: 1.5 pages. Mar 13: 10 pages.
Celebrating 22 Years of Kottke.org
Hello all. I know there’s a pandemic going on out there, but I wanted to take a moment to celebrate kottke.org turning 22 years old today. If you’ve been reading along the entire time or for only a few days, it’s been an honor for me to inform, provoke, entertain, and possibly even infuriate you all for a few minutes every day. Thanks for reading — and an extra-special thanks to those who support the site with a membership. As I said a few weeks ago, all this really means a lot to me.
After cancelling live performances due to COVID-19, NYC’s Metropolitan Opera will be live-streaming opera performances on their site for free. Verdi, Puccini, and Tchaikovsky for starters.
Italy Sings Together During Coronavirus Lockdown
People under quarantine lockdown in Italy due to the country’s COVID-19 outbreak have been singing and playing music out their windows and on their balconies to keep their spirits up while social distancing.
Here’s a Twitter thread with more videos from Salerno, Turin, Naples, Siena, Florence, etc.
No matter how much fear and panic and anxiety and negativity are on display during a crisis, it also brings out the best in people. Humans are social animals and we can’t help sharing with our neighbors, comforting one another, and coming together even when we’re physically apart.
Pandemic Advice from Wu Tang Clan

A message from Wu Tang Clan on Instagram about what to do about the COVID-19 pandemic. This is better guidance than we’re getting from the executive branch of our government. (via maria konnikova)
These guys are assholes, full stop. Cleaning out stores of necessary supplies before the onset of a pandemic is profiteering from human death & suffering and is morally repugnant.
Floodlines, a new podcast from The Atlantic about Hurricane Katrina. Now you can learn about a disaster & relief effort botched by a Republican administration while living through a disaster & relief effort botched by a Republican administration.
This is a clever idea: Quarantine Book Club. Video chats with authors on Zoom, tickets are $5 a pop.
Epidemiologist and former FDA commissioner Dr. David Kessler on what the US government should do to fix the COVID-19 testing mess, e.g. “set up mobile specimen collection units throughout the country, staffed with medics”.
How to Wash Your Hands Properly
Most humans have been washing their hands since childhood, but I bet very few of us have been doing it correctly. Because of the effectiveness of hand-washing with soap in preventing the spread of COVID-19, the CDC and the WHO (and health professionals everywhere) both make it their top recommendation and provide guidance on how to do it properly: CDC hand-washing instructions, WHO hand-washing instructions.
Lather your hands by rubbing them together with the soap. Be sure to lather the backs of your hands, between your fingers, and under your nails. Scrub your hands for at least 20 seconds. Need a timer? Hum the “Happy Birthday” song from beginning to end twice.
Here’s a video from the WHO on proper hand-washing technique (and a similar one from Johns Hopkins that has subtitles):
And a graphic from the WHO:
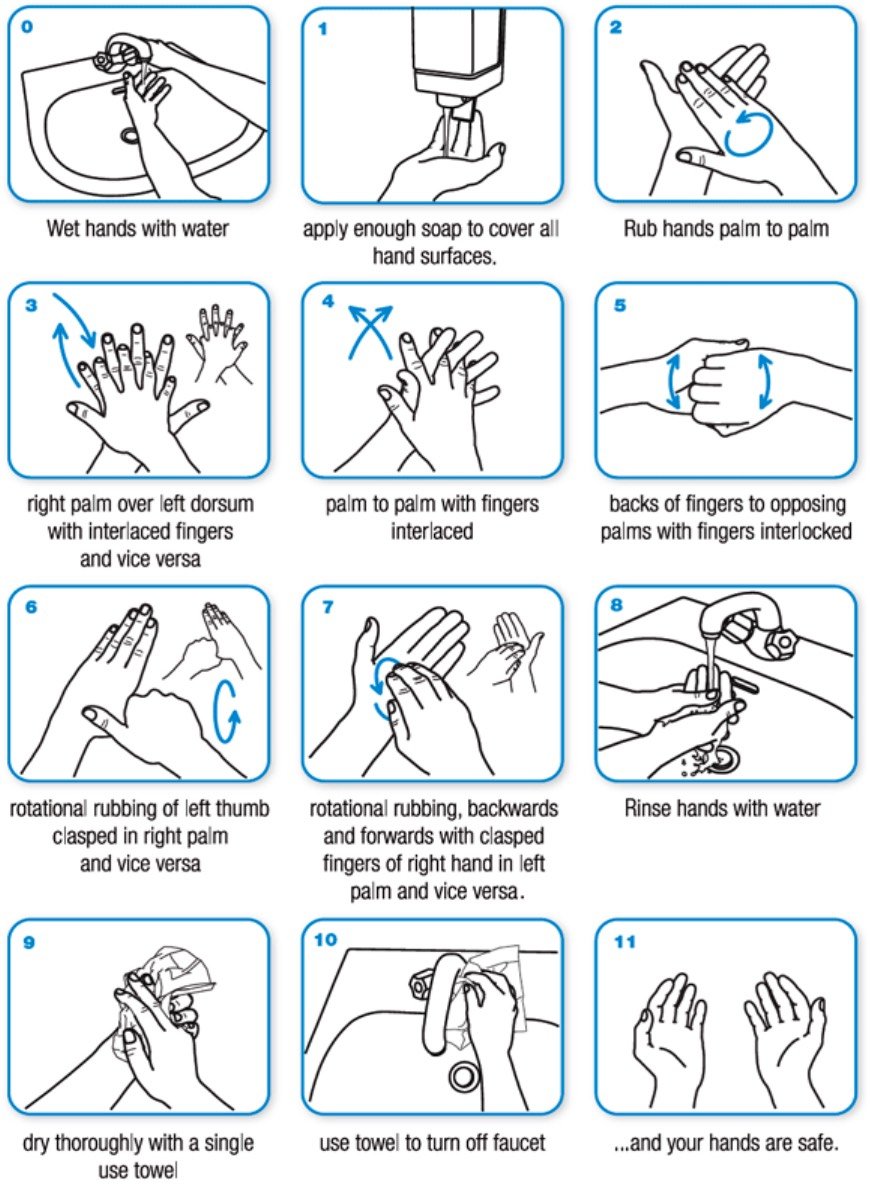
And if you’re getting sick of singing Happy Birthday while washing your hands, a site called Wash Your Lyrics can help you make a hand-washing infographic with your favorite song’s lyrics.
Great interview with Portrait of a Lady on Fire director Céline Sciamma. I saw this earlier in the week and *loved* it.
Why Is the US So Behind in COVID-19 Testing?
According to an ongoing investigation at The Atlantic, the US has tested only about 14,000 people for COVID-19 so far (a stat CDC data seems to confirm). 14,000 out of 330 million people. Olga Khazan writes about the four main reasons why the US is so behind in testing for the virus.
Interviews with laboratory directors and public-health experts reveal a Fyre-Festival-like cascade of problems that have led to a dearth of tests at a time when America desperately needs them. The issues began with onerous requirements for the labs that make the tests, continued because of arcane hurdles that prevented researchers from getting the right supplies, and extended to a White House that seemed to lack cohesion in the pandemic’s early days. Getting out lots of tests for a new disease is a major logistical and scientific challenge, but it can be pulled off with the help of highly efficient, effective government leadership. In this case, such leadership didn’t appear to exist.
Here’s another take on the problem from a few days ago in the NY Times.
The US has bungled the situation so badly that a pair of Chinese foundations announced this morning that they were donating 500,000 testing kits and 1 million masks to the US. Last month in my Asian travelogue, I wrote that my main observation after spending three weeks in Asia was: “America is a rich country that feels like a poor country”. That we have to rely on foreign aid in situations like this is a good example of what I was referring to.
Socials & More